

Translate this page into:
Acute Small Bowel Obstruction Due to Entrapment Under Appendices Epiploicae Tourniquet – Laparoscopic Management

*Corresponding author: Dr. Mounish Raj Nagula, Department of General and Advanced Laparoscopic Surgery, Dr. L H Hiranandani Hospital, Hill Side Avenue, Powai, Mumbai, Maharashtra, India. mounishraj.nagula@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nagula MR, Joshi AS. Acute Small Bowel Obstruction Due to Entrapment Under Appendices Epiploicae Tourniquet – Laparoscopic Management. Int J Recent Surg Med Sci. 2024;10:134-7. doi: 10.25259/IJRSMS_37_2024
Abstract
Epiploic appendagitis is a rare condition in which there is inflammation of the appendices epiploicae (AE). It is rare to see small bowel obstruction due to herniation of the small intestine through adhesion between two adjacent AEs forming a loop. We, herein, present the case of a 64-year old male patient who had presented to us with acute small bowel obstruction. During laparoscopy, the culprit was found to be an internal herniation of an ileal loop between the two AE of the sigmoid colon, which were adherent at their tips. Laparoscopic transection of the tourniquet and excision of the AE was performed, and the patient had an uneventful postoperative recovery.
Keywords
Appendices epiploicae
Intestinal obstruction
Internal hernia
Laparoscopy
Small bowel obstruction
Tourniquet

INTRODUCTION
Acute small bowel obstruction (SBO) is a well-known and common surgical emergency. It is frequently caused by adhesions, hernias, tumors, etc. Ninety percent of SBO cases are caused by them. The remaining 10% of SBO cases are caused by rare conditions like complicated, inflammatory bowel disease, intussusception, post-ischemic stenosis, endometriosis, post-radiation therapy strictures, anastomotic bowel strictures, gallstones, foreign bodies, phytobezoars, and tuberculosis.[1] Inflammation of the AE is a rare and usually self-limiting phenomenon. It is caused by ischemia and/or inflammation of the epiploicae attached to the colon. It usually causes localized abdominal pain. Rarely it leads to adhesion and loop formation. Even rare is the entrapment of the small bowel into such a loop, thereby causing acute obstruction.
CASE REPORT
A 64-year-old male patient presented to the emergency ward with complaints of acute colicky pain all over the abdomen, vomiting, abdominal distension, and obstipation for 12 hours. On examination, his pulse rate was 110 beats per minute, blood pressure was 130/90 mms of Hg, and the respiratory rate was 14 per minute. His abdomen was grossly distended, tympanic, tender, and hyperperistaltic. A per rectal exam revealed an empty rectum. A plain abdominal X-ray showed multiple air-fluid levels all over the abdomen in a characteristic stepladder pattern. A contrast-enhanced computed tomography (CT) scan of the abdomen was then done, and revealed dilated small bowel loops in the central abdomen. An abrupt cutoff was noticed in the right lower abdomen, beyond which there was no passage of oral contrast. A delayed scan done after 12 hours confirmed the findings. He was admitted to the hospital and started on nasogastric tube drainage, intravenous antibiotics, and fluid support. Upon failing an initial trial of conservative management, he was taken up for emergency surgery after due investigational workup. During laparoscopy, he was found to have entrapped and dilated small bowel loops under a loop formed by adherent adjacent AE attached to the sigmoid colon [Figure 1a-d]. The said loop was immediately transected carefully while safeguarding and avoiding iatrogenic injury to the underlying trapped bowel [Figure 2a-d]. A thorough bowel ‘walk’ was then performed from the ileocecal junction to the duodenojejunal flexure to rule out any other pathology/site of obstruction [Figure 3a, b]. The swollen elongated AE were excised [Figure 3c,d and 4a-c]. The peritoneal toilet was then given using normal saline, and 1-litre low molecular weight Dextran was instilled into the peritoneal cavity as a liquid anti-adhesion barrier [Figure 4d]. The patient had an uneventful postoperative recovery. On his post-operative day 10 outpatient department visit, all his wounds had healed well. At the time of writing this report, a telephonic interview was conducted. Thirty months after his surgery, he continues to be symptom-free.
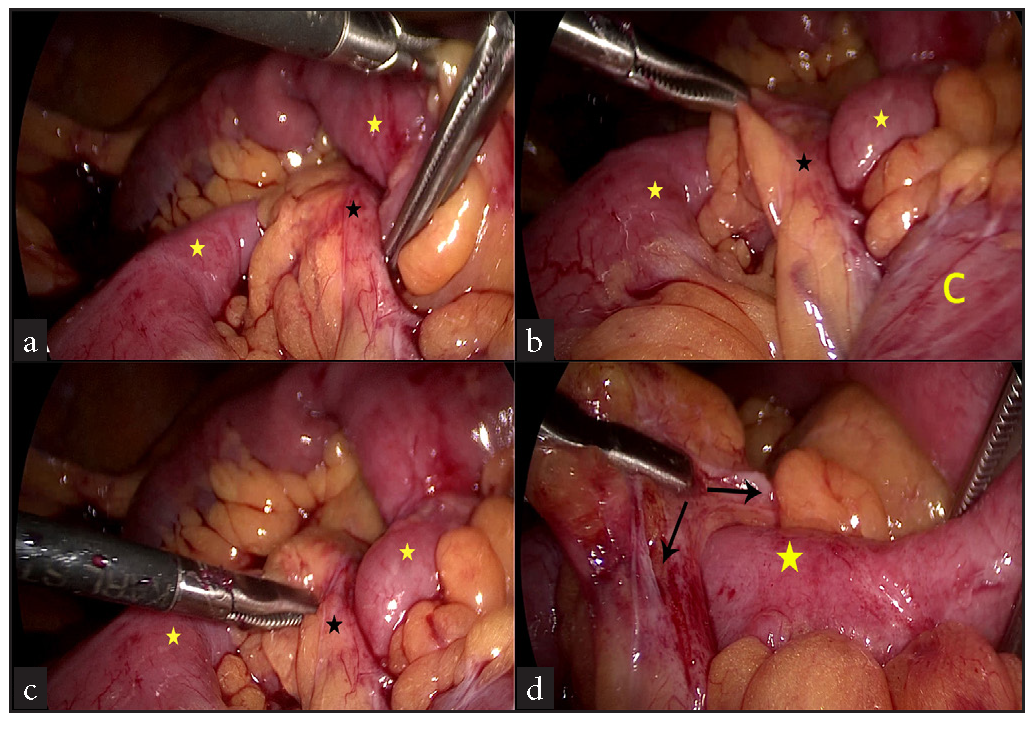
- Operative pics. (a & c) First look appearance of the tourniquet (black asterisks) and small bowel immediately proximal & distal to it (yellow asterisks), (b) loop of sigmoid colon (yellow ‘C’) to which the inflamed elongated appendix epiploica was attached, tourniquet (black asterisks) and small bowel immediately proximal and distal to it (yellow asterisks) (d) Appendices epiploical tourniquet (double headed black arrow) bridging over & extrinsically compressing underlying small bowel (yellow asterisks).
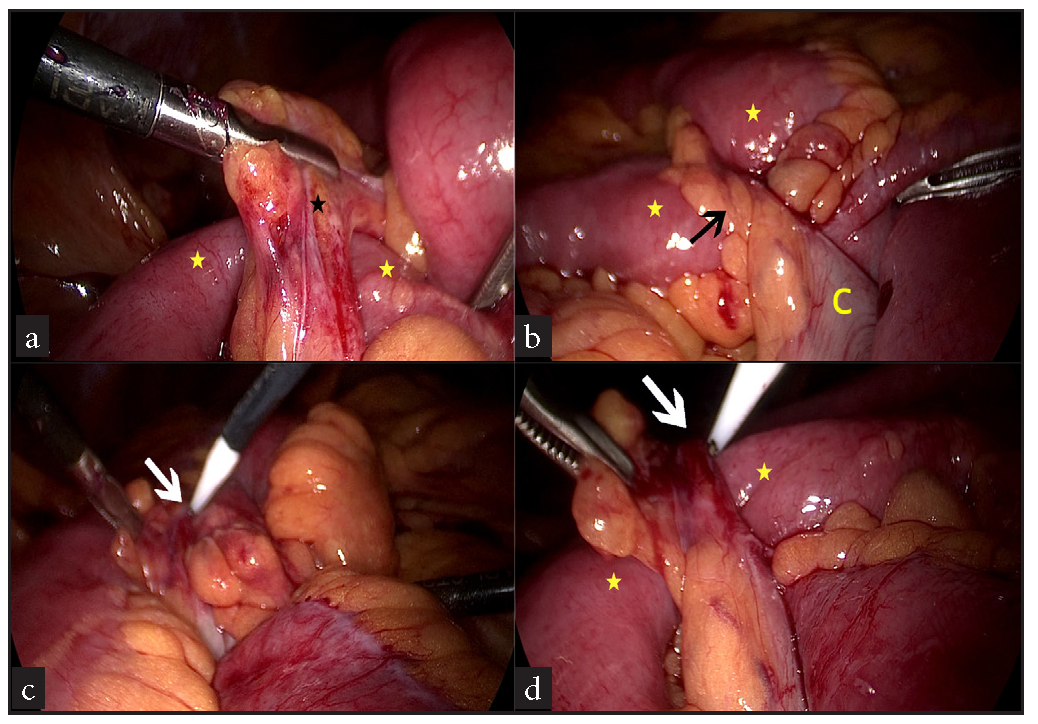
- (a) Culprit obstructing tourniquet (black asterisk) being lifted off the small bowel (yellow asterisks), (b) Epiploical tourniquet (black arrow) attached to sigmoid colon (yellow ‘C’) bridging over and compressing terminal ileum (yellow asterisks), (c,d) Hook with monopolar cautery (white arrows) being used to divide the tourniquet over the ileum (yellow asterisks).
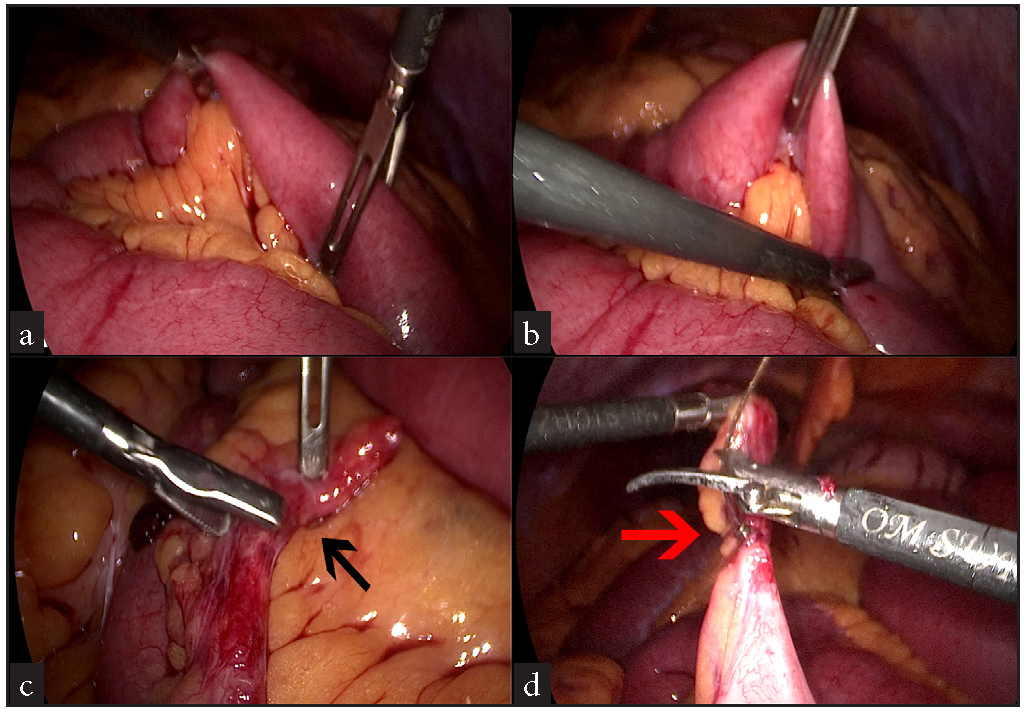
- (a,b) Small bowel ‘walk’ being performed to rule out any other sites of obstruction, (c) Inflamed & elongated tourniquet (black arrow) after division, (d) Ligation of it’s base (red arrow) with Endoloop.
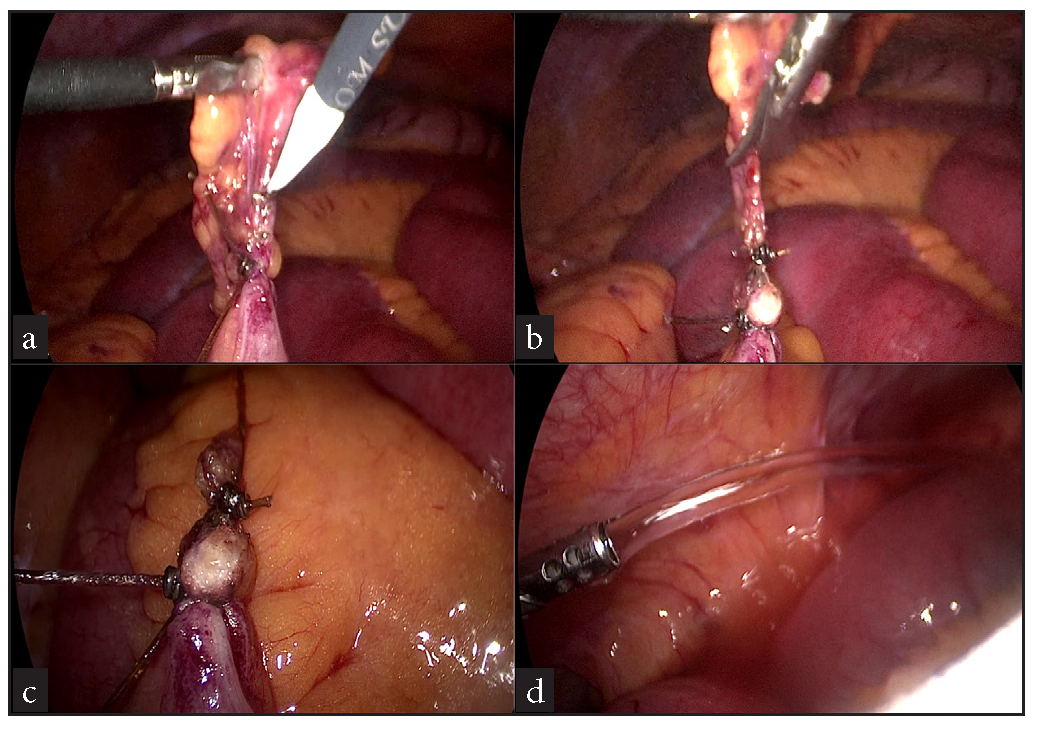
- (a, b) Base of culprit appendix epiploica being transected, (c) Endresult, (d) Local peritoneal toilet being given.
DISCUSSION
Epiploic appendages, also referred to as Appendices epiploicae (AE), are pedunculated adipose tissue structures protruding from the outer surface of the colon and are lined with peritoneum. They comprise lobulated masses of yellow subserosal fat, which have ovoid, grape-like, or oblong finger-like shapes. They are 1-2 cm thick and 0.5-5 cm long. Each AE has one or two arterioles and a venule, which are present in its peduncle.[2] A variety of physiological purposes have been postulated for AE, including the soft and flexible support cushioning of the colon, the role in immune response, and colonic absorption.[3] Approximately 50-100 AE are present in two separate longitudinal rows extending from the caecum to the recto-sigmoid junction.[2] Fifty percent of them are present anteriorly along the taenia libera. The other half is present next to taenia omentalis along the postero-lateral border of the ascending, descending, and sigmoid colon. There is a single row of AE along the transverse colon and none along the rectum.[4] Epiploic appendagitis is a term that indicates inflammation of these AE. Primary epiploic appendagitis (PEA) is rare and most commonly affects obese male patients in their 4th and 5th decades of life. Torsion of the AE is rare but can result in ischemia, which causes an acute abdomen. The clinical picture resembles that of diverticulitis, appendicitis, or other more serious causes of acute abdominal pain.[5] Apart from torsion, spontaneous thrombosis of the draining vein of the AE is another rare cause of PEA.[6] A torsion leading to infarction of the AE is most frequently observed in the sigmoid colon (41.5%) and the caecum (15.1%), as these stretches usually harbor the most prominent and elongated AE.[7] Spontaneous thrombosis of an appendageal vein is another cause of EA.[6] Also, EA could be secondarily caused just by contiguity due to its proximity to inflamed organs like the colon (diverticulitis), appendix (appendicitis), gallbladder (cholecystitis), or pancreas.[8] The calculated incidence of EA is said to be 8.8 per million people per year.[9] A high-attenuation focus within the inflamed AE noted on CT, has been reported as “the central dot sign.” This may be appreciated in the emergency setting.[10] PEA is considered a self-limiting pathology and is usually treated non-operatively with analgesics, occasionally complemented by nonsteroidal anti-inflammatory drugs (NSAIDS).[11] If symptoms remain or recur, surgical excision of the concerned AE is considered as definitive therapy. An internal herniation involving AE is possible and happens because of the inflammation causing adhesions between adjacent AE or between AE and the adjoining structures. Such adhesions can occur even in the absence of a previous history of abdominal surgery.
Internal hernias are rare phenomena, and the incidence of intestinal obstruction caused by internal hernia is just 0.2–0.9% of all cases of intestinal obstruction.[12] A high index of suspicion with prompt intervention often saves lives. Radiology can help to prove the diagnosis and indicate the level of obstruction. Mild inflammation in the appendices in this patient might have led to adhesion and herniation, leading to an SBO. A review of English language literature revealed that only 7 cases of an AE tourniquet causing SBO over the last 10 years worldwide [Table 1]. Also, only two such patients have been managed by laparoscopy throughout history.[13,14] Thus, to the best of our knowledge, this is only the third successfully laparoscopically managed and reported case of all time in world literature.
| Author | Yr. of publication/Age (in years)/Sex | Contents of the internal hernia | Mode of surgery | Condition of entrapped bowel |
|---|---|---|---|---|
| Suzuki Y et al.[13] | 2015 | Ileum | Single incision laparoscopic surgery (SILS) | Viable |
| Srivastava KN et al.[14] | 2018/75/M | Ileum | Open | Viable |
| Butt M et al.[15] | 2021/48/ M | Ileum | Laparoscopy | Viable |
| Hadjizacharias T et al.[16] | 2020/69/M | Ileum | Open | Viable |
| Thomas Olagboyega Olajide[17] | 2020/64/F | Ileum | Open | Gangrenous |
| Zabihi F et al.[18] | 2022/87/F | Ileum | Open | Viable |
| Ghali MS et al.[19] | 2024/58/M | Ileum | Open | Gangrenous |
AE: Appendices epiploicae, SBO: Small bowel obstruction
CONCLUSION
As seen in this report, acute SBO occurring due to internal herniation through the adhesions between adjoining appendices is known and reported, albeit a very rare event. Also, as seen here, even acute SBO caused by this rarest of rare internal herniation can be managed by laparoscopy in an advanced setup complimented by advanced laparoscopic surgical skills.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
REFERENCES
- Vascular Loops in the Appendices Epiploicae; Their Anatomy and Surgical Significance, with a Review of the Surgical Pathology of Appendices Epiploicae. Br J Surg. 1950;37:464-6.
- [CrossRef] [PubMed] [Google Scholar]
- Primary Inflammation of the Appendices Epiploicae: With Review of the Literature and Report of Six Additional Cases. Ann Surg. 1949;129:533-7.
- [CrossRef] [PubMed] [Google Scholar]
- Epiploic Appendage. Reference Article, Radiopaedia.org [accessed on 2024 Aug 1] https://doi.org/10.53347/rID-26187
- Epiploic Appendagitis--Clinical Characteristics of an Uncommon Surgical Diagnosis. BMC Surg. 2007;7:11.
- [CrossRef] [PubMed] [Google Scholar]
- Epiploic Appendagitis: The Emergency Department Presentation. J Emerg Med.. 2002;22:9-13.
- [CrossRef] [PubMed] [Google Scholar]
- Appendices Epiploicae of the Colon: Radiologic and Pathologic Features. Radiographics. 1992;12:59-77.
- [CrossRef] [PubMed] [Google Scholar]
- Epiploic Appendagitis: An Entity Frequently Unknown to Clinicians--Diagnostic Imaging, Pitfalls, and Look-alikes. AJR Am J Roentgenol. 2009;193:1243-51.
- [CrossRef] [PubMed] [Google Scholar]
- Fréquence et épidémiologie descriptive de l’appendiciteépiploïque primitive par l’explorationto modensitométrique des douleursabdominales de l’adulte [Frequency and Epidemiology of Primary Epiploic Appendagitis on CT in Adults with Abdominal Pain] J Radiol. 2008;89:235-43.
- [CrossRef] [PubMed] [Google Scholar]
- CT Imaging Findings of Epiploic Appendagitis: An Unusual Cause of Abdominal Pain. Insights Imaging. 2019;10:26.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Epiploic Appendagitis: Pathogenesis, Clinical Findings and Imaging Clues of a Misdiagnosed Mimicker. Ann Transl Med. 2019;7:814.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Internal Hernia: Clinical and Imaging Findings in 17 Patients with Emphasis on CT Criteria. Radiology. 2001;218:68-74.
- [CrossRef] [PubMed] [Google Scholar]
- Internal Hernia Caused by Epiploic Appendices Successfully Treated by Single-incision Laparoscopic Surgery (SILS) Hernia. 2015;19:1011-3.
- [CrossRef] [PubMed] [Google Scholar]
- An Unusual Case of Intestinal Obstruction Due to Internal Herniation from Adhesions Between Two Appendices Epiploicae. J Surg Case Rep. 2018;2018:rjy239.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Rare Cause of Small Bowel Obstruction Secondary to Epiploic Appendagitis: Diagnostic Dilemma and Role of Minimal Invasive Surgery. Int J Surg Case Rep. 2021;78:30-3.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Epiploic Appendagitis Causing Small Bowel Obstruction: A Pleasant Surprise. Case Rep Surg. 2020;2020:3126495.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A Rare Case of Intestinal Obstruction from Internal Hernia Through a Foramen Formed by Appendices Epiploicae-A case Report and Review of Literature. Open Access Maced J Med Sci. 2020;8:4-6.
- [Google Scholar]
- Two Connected Large Epiploic Appendixes Make a Loop: A Case Report. Clin Case Rep. 2022;10:e6119.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Uncommon Presentation of Complicated Internal Hernia Through the Appendices Epiploicae Ring of Adhesion: A Clinical Case Study. Front Surg. 2024;10:1288369.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




