

Translate this page into:
Atraumatic Isolated Bilateral Fibular Shaft Fragility Fracture: A Rare Case
*Corresponding author: Akash Kumar, Department of Orthopaedics, Karnataka Institute of Medical Sciences, Vidya Nagar, Hubli, Karnataka, India. akasha856@gmail.com
Abstract
Fragility fractures, a form of stress fracture brought on by physiological stress on weak bones, are not common. It might be challenging to diagnose a fragility fracture since a standard radiograph shows signs of fracture repair rather than the actual fracture. We present a case of a 32-year-old woman who has been complaining of both leg pain for the last 4 months and has been unable to stand for the last 1 week. Further analysis revealed that her vitamin D levels were insufficient.
Keywords
Fragility fracture
Stress fracture
Osteomalacia
Fibula osteopenia

Introduction
Stress fractures are thought to be the result of continual stress on the bone rather than an acute traumatic occurrence.[1] They can be seen in athletes, most likely as a result of the constant stress on bone caused by exertion. Fragility fractures develop as a result of normal stress on the defective or inadequate bone. Certain areas of preference include the vertebra, pelvis, sacrum, ribs, the distal end of the ulna, and, to a lesser extent, the proximal and distal end of the tibia and fibula.[2–4] So far, just one isolated bilateral fibula insufficiency fracture without deformity has been recorded in English literature.[5] We describe an interesting case of fragility fracture in a younger patient.
Case Report
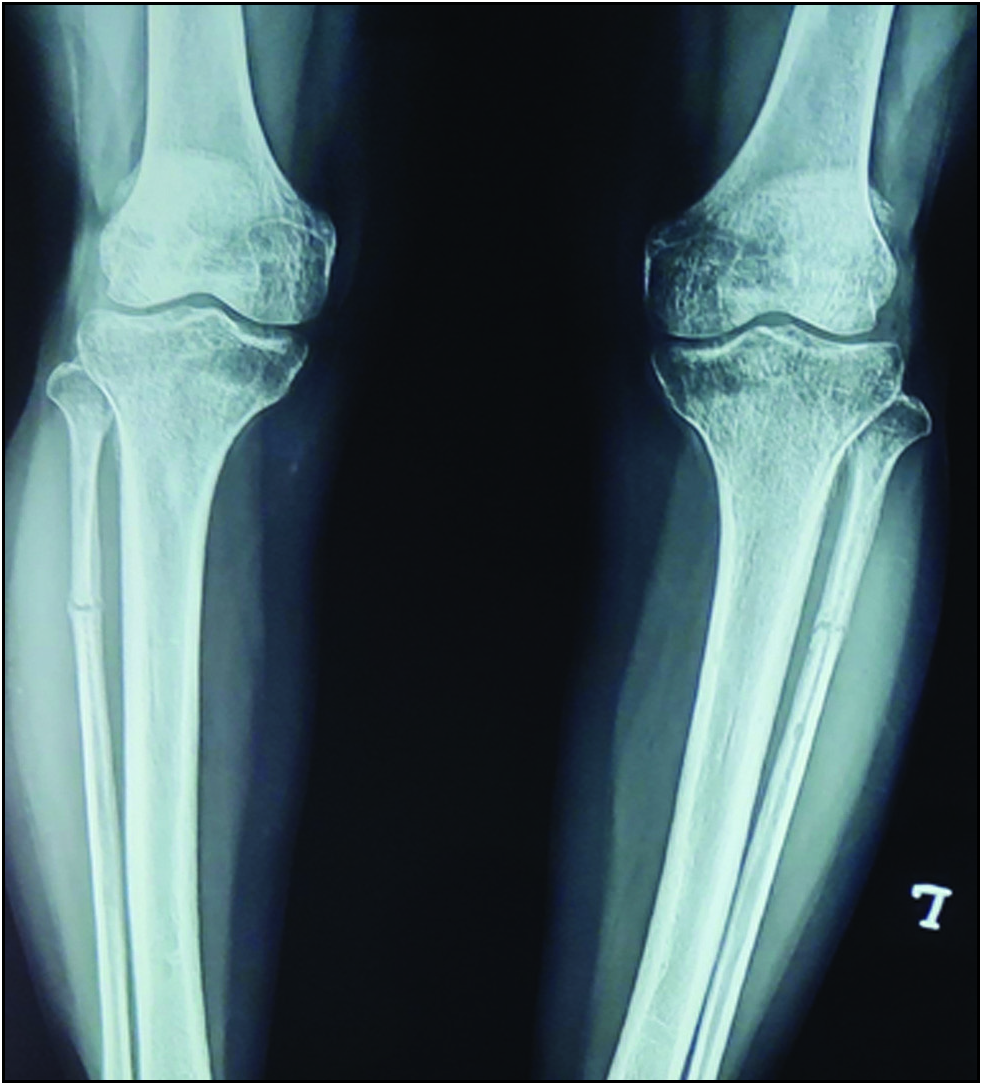
A 32-year-old woman presented to our orthopaedic outpatient department with a complaint of both leg pain for the last 4 months and has been unable to stand for the last 1 week. The pain is continuous and not relieved by rest. There was no associated history of recent trauma. She was a housewife and had no history of participating in strenuous exercise like running or playing sports. She was previously seen by a neurosurgeon and treated with neurogenic claudication for 3 weeks for her symptoms. Her symptoms were not relieved and refereed to our orthopaedics department. There was tenderness present on anterior lateral aspect of proximal leg and varus deformity of both knees. No swelling or limitations on mobility was found. The patient did not mention having ever had joint discomfort. Evidence of a transversely orientated, undisplaced fracture in the right as well as left fibular shaft was seen on the radiograph of both knees with the leg [Figure 1]. Apart from the site being slightly more proximally on the left, the fractures looked to be extremely comparable. Periarticular osteopenia, tibial metaphyseal varus deformity, and reduced lateral joint space of knee joint were found on examination. The patient was questioned once again regarding distant insignificant trauma, but she was unable to remember. Routine investigations like complete blood count, erythrocyte sedimentation rate, rheumatoid factor, C-reactive protein and blood, uric acids, liver function test, kidney function test, lactate dehydrogenase, thyroid profile, vitamin D3, and parathyroid hormone were normal. Given that vitamin D deficiency is widespread in India, she was tested and found to have hypovitaminosis D (24.1 ng/mL). Her serum calcium level was borderline, at 9 mg%. Since no other cause for the fracture was found, the patient was started on oral vitamin D therapy (oral cholecalciferol 60,000 IU once a week for 6 weeks and calcium supplements), as well as an above knee slab was applied and weight bearing restrictions for 6 weeks was advised. After 6 weeks of treatment, a repeated X-ray [Figure 2] showed callus formation around the fracture line, and the patient mobilized with partial weight bearing with a walker.

- X-ray at the time of presentation.
- Six-week follow-up X-ray.
Discussion
Normal or physiological muscle action exerts stress on bone that lacks mineral or elastic resistance, resulting in fragility fractures.[2] Fragility fractures become more common as people become older. They are more common in women and occur at trabecular bone-rich locations. Young people with underlying bone-weakening illnesses including osteoporosis, chronic inflammatory diseases like rheumatoid arthritis, vitamin D insufficiency, hyperparathyroidism, endocrine disorders, and chronic renal failure can also suffer from fragility fractures.[2],[6–7] Only 6 to 16% of the stress delivered from the lower extremity is received by the fibula. Radiographs in the early stages are usually normal. During the healing process, new bone and fracture lines become visible. Healing bone’s profuse callus production mimics periosteal new bone tumor and infection. A fibula stress fracture is indicated by a triad of bowed fibula periosteal thickening, a transverse region of radiolucency, and/or sclerosis on radiograph. The radionuclide bone scan invariably shows localized enhanced radiotracer uptake at the locations of these fractures in the early stages of stress fracture.[8]
The most sensitive is magnetic resonance imaging that is precise method for determining the occurrence of periosteal and bone marrow edema in stress fractures at an early stage.[9] The treatment of choices for fragility future is conservative and consists mainly vitamin D of sachets 60,000 IU once a weekly for 6 weeks, supplementation of calcium, analgesia, and immobilization. Management of the underlying cause is essential to prevent recurrence.
The Goal of Learning
-
It is quite unusual to have a spontaneous atraumatic isolated bilateral fibular fracture.
-
Radiographs demonstrate periarticular osteopenia, a narrowed lateral joint space, and a tibial metaphyseal varus deformity.
-
In our situation, we had an atraumatic isolated fibular fracture with a stress fracture owing to a vitamin D insufficiency.
Funding
None.
Conflict of interest
None.
References
- Bilateral symmetric stress fractures in a toddler. J Pediatr Orthop B. 2001;10:73-77. [PubMed]
- [PubMed] [Google Scholar]
- Insufficiency fractures at unusual sites: a case series. J Orthop Case Rep. 2017;7:76-9.
- [Google Scholar]
- Imaging features and management of stress, atypical, and pathologic fractures. Radiographics. 2018;38:2173-92.
- [CrossRef] [PubMed] [Google Scholar]
- Insufficiency fractures of the tibia and fibula. Semin Arthritis Rheum. 1999;28:413-20.
- [Google Scholar]
- Isolated bilateral fibular insufficiency fractures: case report of an unusual entity. J Clin Orthop Trauma. 2022;35:102066.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Imaging of insufficiency fractures. Eur J Radiol. 2009;71:398-405.
- [CrossRef] [PubMed] [Google Scholar]
- Insufficiency fracture. A survey of 60 cases and review of the literature. Joint Bone Spine. 2003;70:209-18.
- [CrossRef] [PubMed] [Google Scholar]
- Atypical healed stress fracture of the fibula masquerading as chronic osteomyelitis. A case report of magnetic resonance distinction. Am J Sports Med. 1988;16:185-8. [PubMed]
- [CrossRef] [PubMed] [Google Scholar]
- Stress fractures of the fibula in the first few years of life (report of six cases) Australas Radiol. 1996;40:261-3. [PubMed]
- [CrossRef] [PubMed] [Google Scholar]




