

Translate this page into:
Surgical Audit of Operated Patients in a Tertiary Care Hospital in Karachi, Pakistan

*Corresponding author: Dr. Huma Akhtar, Department of General Surgery, Surgical Unit II, Abbasi Shaheed Hospital and Karachi Medical and Dental College, Karachi, Pakistan. huma1345@hotmail.com
-
Received: ,
Accepted: ,
How to cite this article: Akhtar H, Ahmed HH, Irshad K, Jamaluddin M. Surgical Audit of Operated Patients in a Tertiary Care Hospital in Karachi, Pakistan. Int J Recent Sur Med Sci. 2023;9:97-104. doi: 10.25259/IJRSMS-2020-12-4.
Abstract
Objectives
To audit operated patients in emergency and electively from 1st January 2018 to 31st December 2019 in all three surgical departments to know the outcome of the patients at a tertiary care hospital in Karachi, Pakistan.
Material and Methods
A retrospective study conducted in all three Abbasi Shaheed Hospital surgical units from 1st January 2018 to 31st December 2019. In this study total of 5079 patients were included who were admitted through the emergency and surgical outpatient department. They were operated in emergency and elective theaters in all three surgical departments of Abbasi Shaheed Hospital. Data was collected on pre-designed performa from emergency and elective theater, wards, High-dependency unit and Intensive care unit maintained registers by staff.
Results
A total of 5079 cases were operated during January 2018 to December 2019. Among all the age ranges 1282 belongs to the age range of 21-30 years. Amongst which 59.6% were males. The most common diagnosis made in elective patients was chronic calculous cholecystitis (25.8%) and an abscess in emergency (39.4%). The most common procedure performed in elective surgeries was combined laparoscopic and open cholecystectomy (26.8%) and incision and drainage in the emergency (39.4%). Elective surgeries were mainly performed by Associate Professors (28.7). While, emergency surgeries were mainly performed by post-graduate trainees (70.2%). Surgical unit II has performed most surgeries (39.5%). Elective procedure constitutes about (51.60%). Total 19 patients expired out of 350 patients who were shifted or admitted in surgical ICU and 12 patients expired in all three wards.
Conclusion
We have a higher number of elective surgeries as compared to the emergency surgeries. Consultants have performed most of the elective surgeries. Emergency surgeries mostly by residents and senior registrars. We have zero mortalities in our elective surgeries in comparison with emergency surgeries. We call attention to conduct continuous audits at our hospitals and all levels of health care and demand from higher authorized personnels to incorporate audit awareness in our teaching. Along with it, a proper database should be installed with updated records maintenance to improve the lack of health care.
Keywords
Surgical Audit
Elective Surgery
Emergency Surgery
Tertiary Care

Introduction
An audit is derived from the Latin word “Audire”, meaning “to hear”.[1]
“Clinical audit is a quality improvement process that seeks to improve patient care and outcomes through a systematic review of care against explicit criteria and the review of change. Aspects of the structure, process and outcome of care are selected and systematically evaluated against explicit criteria. Where indicated changes are implemented at an individual, team, or service level, further monitoring is used to confirm improvement in healthcare delivery.” (National Institute of Health and Care Excellence (NICE), 2002).[2]
Patient care can be gauged from the outcomes, ultimately assessing the health care systems. The backbone of quality improvement of the health care system is audits, which should preferably be carried out systematically instead of infrequently.[3]
Continuous systematic audit has many advantages, including promoting good professional practice with proven methodologies, the correlation between the best use of resources and increasing efficiency, and improvement in training, education and the overall health system. An audit conducted by health care professionals is termed a clinical audit.[4]
Clinical audit is a valuable part of developed countries and is used to identify and improve the deficiencies in daily practice, unlike developing countries.[5] Perpetual systemic audits carry multitudinous prerogative comprised of encouragement of good professional practice with tried and tested methodologies, how to utilize the resources and make use of it in increasing the efficiency, improvement in training, education methodologies and altogether health care system.[6] Audit convened by health care professionals entitled as a clinical audit.[7] Audit results can be used to conduct essential research, which can be projected on the whole community.[8] Audit judges the performance of the surgical team and their procedures. An audit is a crucial part of health care as it adds up new thinking ways and modalities in research audit needs to be addressed, especially in developing countries. Many surgical procedures still being done in developing countries are obsolete now. Organizations of audits can evaluate the benefits and drawbacks of obsolete procedures. Healthcare workers should take an interest in audits and research activities.[9]
A historical review of audits shows that the objective and role of auditors are constantly evolving.[10] Developing countries should conduct clinical audits regularly to determine the lack of routine clinical practice and improve them like developed countries. It is, therefore, time to ratify audit as an essential part of research methodology. Audits can highly improve the evaluation of health care management’s structure, process and outcome. They should be incorporated in all health care professionals’ programs and tiers. It will help enhance the system to work with standard-based medicine with timely updates of guidelines and standards.
This audit aims to report the number of surgeries performed in a tertiary care public sector hospital and considering the outcome improvement that can be done in providing health care.
Material and Methods
We conducted an observational retrospective descriptive study in three Abbasi Shaheed Hospital Karachi surgical departments. In this study, an audit of 5079 cases operated in emergency and elective of all three surgical units at Abbasi Shaheed Hospital Karachi was done. There are three surgical units in Abbasi Shaheed Hospital. Each unit covers an emergency twice a week, with one special Sunday. The study duration was from 1st January 2018 to 31st December 2019. Data was collected on a pre-designed performa from the emergency, elective theater, wards, high dependency unit and intensive care units. Records were maintained in handwritten journals by respective paramedical staff. Details consisting of age, gender, diagnosis, operative procedure, level of the surgeon, unit and whether the procedure was performed in an emergency or elective were recorded. We also collected data on mortalities from wards, ICU and HDU. Sampling was consecutive, non-probability sampling. Inclusion criteria included patients operating in the general surgical department in emergency and elective theaters. Exclusion criteria were operated patients in other surgical departments like Orthopaedics, ENT, Neurosurgery, Plastics and Burns surgery and Urology, patients from minor operation theater, combined surgeries and patients who were operated outside Abbasi Shaheed Hospital and shifted to the surgical department for further management. The data was entered and analyzed on the computer using SPSS Version 26.
RESULTS
A total of 5079 cases were operated from 1st January 2018 to 31st December 2019. Among 0 to 100 years total of 1282 patients belongs to the age range of 21-30 years, as shown in Table 1. Amongst these, male dominancy of 59.6% was noted, as shown in Table 2. The most common diagnosis in elective patients was chronic calculous cholecystitis accounting for 25.8%, followed by inguinal hernia at 18.2% and fibroadenoma at 5.8%, shown in Table 3. In an emergency, an abscess was the most commonly made diagnosis accounting for 39.4%, followed by acute appendicitis at 33.0% and generalized peritonitis 13.5%, as shown in Table 4. The most common procedure in elective surgeries was cholecystectomy, including both laparoscopic and open technique, each accounting for 19.8% and 6% making 25.8%, followed by mesh repair of hernia 24.2% and excision and biopsy 8.7% shown in Table 5. Incision and drainage was the most common emergency surgery, accounting for 39.4%, followed by open appendicectomy at 33.0% and exploratory laparotomy at 15.9%, as shown in Table 6. We also looked for surgeons’ levels in elective and emergency cases. Elective theater associate professors have performed the highest number of surgeries, accounting for 28.7% shown in Table 7 and Figure 1. Meanwhile, surgeries in the emergency theater were mostly done by post-graduate trainees accounting for 70.2% shown in Table 8 and Figure 2. Most surgeries, including elective and emergency, were performed in surgical unit 2 around 39.5%, followed by surgical unit I around 35.68% and surgical unit III about 24.81%, as shown in Table 9 and Figure 3. Out of 5079 cases operated, elective procedures constitute about 51.60% and emergency about 48.40% as shown in Table 10 and Figure 4. Total, 350 patients were shifted to or admitted to a surgical intensive care unit, of which 93 patients The most common reason for death was trauma secondary to firearm injury, stab wound and road traffic accident. A total of 12 patients expired in all three wards. The mortality percentage in two-years was 2.067%.
| Age range | Frequency | Percent |
|---|---|---|
| 0–10 | 216 | 4.3 |
| 11–20 | 1078 | 21.2 |
| 21–30 | 1282 | 25.2 |
| 31–40 | 1039 | 20.5 |
| 41–50 | 744 | 14.6 |
| 51–60 | 460 | 9.1 |
| 61–70 | 199 | 3.9 |
| 71–80 | 50 | 1.0 |
| 81–90 | 10 | .2 |
| 91–100 | 1 | .0 |
| Total | 5079 | 100.0 |
| Gender | Frequency | Percent |
|---|---|---|
| Male | 2893 | 57.0 |
| Female | 2186 | 43.0 |
| Total | 5079 | 100.0 |
| Elective diagnosis | Frequency | Percent |
|---|---|---|
| Chronic Calculous Cholecystitis | 676 | 25.8 |
| Inguinal Hernia | 478 | 18.2 |
| Fibroadenoma | 153 | 5.8 |
| Low Fistula in Ano | 126 | 4.8 |
| Paraumbilical Hernia | 95 | 3.6 |
| Third Degree Haemorrhoids | 88 | 3.4 |
| Acute Appendicitis | 70 | 2.7 |
| Patent Processus Vaginalis | 69 | 2.6 |
| Lymphadenopathy | 61 | 2.3 |
| Incisional Hernia | 55 | 2.1 |
| Fissure in Ano | 49 | 1.9 |
| Lipoma | 46 | 1.8 |
| Rectal Polyp | 42 | 1.6 |
| Accessory Breast | 39 | 1.5 |
| Hydrocele | 37 | 1.4 |
| Bowel Reversal | 35 | 1.3 |
| Epigastric Hernia | 35 | 1.3 |
| High Fistula in Ano | 35 | 1.3 |
| Sebaceous Cyst | 33 | 1.3 |
| Pilonidal Sinus | 28 | 1.1 |
| Intact Foreskin of Penis | 26 | 1 |
| Intestinal Obstruction | 25 | 1 |
| Per-Rectal bleed | 22 | 0.8 |
| Umbilical Hernia | 20 | 0.8 |
| Varicose Veins | 19 | 0.7 |
| Epigastric Pain | 17 | 0.6 |
| Sinus | 15 | 0.6 |
| Port-site Hernia | 14 | 0.5 |
| Thyroid Nodule | 14 | 0.5 |
| Carcinoma Breast | 13 | 0.5 |
| Chronic Diarrhea | 13 | 0.5 |
| Gastritis | 12 | 0.5 |
| Pyogenic Granuloma | 12 | 0.5 |
| Varicocele | 12 | 0.5 |
| Gastroesophageal Reflux Disease | 11 | 0.4 |
| Undescended Testis | 10 | 0.4 |
| Multinodular Thyroid | 8 | 0.3 |
| Dysphagia | 7 | 0.3 |
| Gastric Outlet Obstruction | 6 | 0.2 |
| Ganglion Cyst | 6 | 0.2 |
| Epididymal Cyst | 6 | 0.2 |
| Dermoid Cyst | 5 | 0.2 |
| Phimosis | 5 | 0.2 |
| Hidradenitis Suppurativa | 4 | 0.2 |
| Colon Carcinoma | 3 | 0.1 |
| Iron Deficiency Anaemia | 3 | 0.1 |
| Carcinoma Sigmoid Colon | 3 | 0.1 |
| Ovarian Mass | 3 | 0.1 |
| Carcinoma Esophagus | 3 | 0.1 |
| Suture Granuloma | 3 | 0.1 |
| Hemangioma | 3 | 0.1 |
| Parotid Tumor | 3 | 0.1 |
| Esophageal Mass | 2 | 0.1 |
| Sigmoid Mass | 2 | 0.1 |
| Inflammatory Bowel Disease | 2 | 0.1 |
| Femoral Hernia | 1 | 0 |
| Myopathy | 1 | 0 |
| Endometriosis | 1 | 0 |
| Carcinoma Arm | 1 | 0 |
| Hydatid Cyst | 1 | 0 |
| Retractile Testis | 1 | 0 |
| Adrenal Mass | 1 | 0 |
| Ovarian Cyst | 1 | 0 |
| Thyroglossal Fistula | 1 | 0 |
| Rectal Prolapse | 1 | 0 |
| Revision Colostomy | 1 | 0 |
| Brachial Artery Thrombosis | 1 | 0 |
| Idiopathic Thrombocytopenic Purpura | 1 | 0 |
| Total | 2621 | 100 |
| Rectal Carcinoma | 2 | 0.1 |
| Cystic Hygroma | 2 | 0.1 |
| Galactocele | 2 | 0.1 |
| Carcinoma Oral Cavity | 2 | 0.1 |
| Papilloma | 2 | 0.1 |
| Hematemesis | 2 | 0.1 |
| Primary Infertility | 2 | 0.1 |
| Testicular Tumor | 2 | 0.1 |
| Acid Peptic Disease | 1 | 0 |
| Sliding Hiatal Hernia | 1 | 0 |
| Pseudopancreatic Cyst | 1 | 0 |
| Perforated Gall Bladder | 1 | 0 |
| Carcinoma Anal Canal | 1 | 0 |
| Intussusception | 1 | 0 |
| Branchial Cyst | 1 | 0 |
| Thyroglossal Cyst | 1 | 0 |
| Stomal Hernia | 1 | 0 |
| Carcinoma Pancreas | 1 | 0 |
| Emergency diagnosis | Frequency | Percent |
|---|---|---|
| Abscess | 969 | 39.4 |
| Acute Appendicitis | 811 | 33.0 |
| Peritonitis | 333 | 13.5 |
| Carbuncle | 69 | 2.8 |
| Firearm Injury to Abdomen | 58 | 2.4 |
| Hemothorax/Pneumothorax | 52 | 2.1 |
| Glass Cut Injury | 42 | 1.7 |
| Inguinal Hernia | 39 | 1.6 |
| Necrotic Patch | 34 | 1.4 |
| Testicular Torsion | 22 | .9 |
| Compartment Syndrome | 10 | .4 |
| Para-umbilical Hernia | 7 | .3 |
| Carcinoma Oral Cavity | 4 | .2 |
| Carcinoma Esophagus | 4 | .2 |
| Rectal Polyp | 2 | .1 |
| Pilonidal Sinus | 2 | .1 |
| Total | 2458 | 100.0 |
| Procedure | Frequency | Percent |
|---|---|---|
| Mesh Repair by Open Technique | 635 | 24.2 |
| Laparoscopic Cholecystectomy | 518 | 19.8 |
| Excision and Biopsy | 228 | 8.7 |
| Open Cholecystectomy | 158 | 6 |
| Excision and Biopsy | 153 | 5.8 |
| Herniotomy | 133 | 5.1 |
| Fistulotomy | 126 | 4.8 |
| Haemorrhoidectomy | 88 | 3.4 |
| Upper Gastrointestinal Endoscopy | 58 | 2.2 |
| Lateral Sphincterotomy | 49 | 1.9 |
| Excision of Sinus Tract | 43 | 1.6 |
| Polypectomy | 42 | 1.6 |
| Open Appendectomy | 42 | 1.6 |
| Exploratory Laparotomy | 40 | 1.5 |
| Seton Placement | 35 | 1.3 |
| Lower Gastrointestinal Endoscopy | 35 | 1.3 |
| Jabouley’s Procedure | 33 | 1.3 |
| Ileostomy Reversal | 32 | 1.2 |
| Laparoscopic Appendectomy | 28 | 1.1 |
| Stripping and Ligation of Long Saphenous Vein with Avulsion of Small Tributaries | 19 | 0.7 |
| Circumcision by Open Method | 16 | 0.6 |
| Circumcision by Bell Method | 15 | 0.6 |
| Thyroid Lobectomy | 15 | 0.6 |
| Modified Radical Mastectomy | 11 | 0.4 |
| Low Ligation | 10 | 0.4 |
| Orchidopexy | 8 | 0.3 |
| Sigmoidoscopy | 7 | 0.3 |
| Gastrostomy | 5 | 0.2 |
| Total Thyroidectomy | 5 | 0.2 |
| Orchidectomy | 5 | 0.2 |
| Lords procedure | 4 | 0.2 |
| Biopsy | 4 | 0.2 |
| Colostomy Reversal | 3 | 0.1 |
| Superficial Parotidectomy | 3 | 0.1 |
| Toilet Mastectomy | 2 | 0.1 |
| Sub-total Thyroidectomy | 2 | 0.1 |
| High Ligation | 2 | 0.1 |
| Laparoscopic Removal | 2 | 0.1 |
| Distal Pancreatectomy | 1 | 0 |
| Sistrunk Operation | 1 | 0 |
| Abdominal Perineal Resection | 1 | 0 |
| Abdominal Rectopexy | 1 | 0 |
| Revision Colostomy | 1 | 0 |
| Bypass Procedure of Brachial Artery Thrombosis | 1 | 0 |
| Splenectomy | 1 | 0 |
| Total | 2621 | 100 |
| Emergency procedure | Frequency | Percent |
|---|---|---|
| Incision and Drainage | 969 | 39.4 |
| Open Appendectomy | 811 | 33.0 |
| Exploratory Laparotomy | 391 | 15.9 |
| Wound Debridement | 103 | 4.2 |
| Tube Thoracostomy | 52 | 2.1 |
| Herniotomy | 46 | 1.9 |
| Main Arterial Repair/Ligation of Small Branches/Hemostasis Secured of Muscle Bleed | 42 | 1.7 |
| Orchidopexy | 16 | .7 |
| Fasciotomy | 10 | .4 |
| Gastrostomy | 8 | .3 |
| Orchidectomy | 6 | .2 |
| Polypectomy | 2 | .1 |
| Excision of Sinus Tract | 2 | .1 |
| Total | 2458 | 100.0 |
| Level of a surgeon in elective | Frequency | Percent |
|---|---|---|
| Associate Professor | 751 | 28.7 |
| Professor | 486 | 18.5 |
| Postgraduate Trainee | 423 | 16.1 |
| Assistant Professor | 389 | 14.8 |
| Senior Registrar | 388 | 14.8 |
| Resident Medical Officer | 182 | 6.9 |
| House Officer | 2 | .1 |
| Total | 2621 | 100.0 |
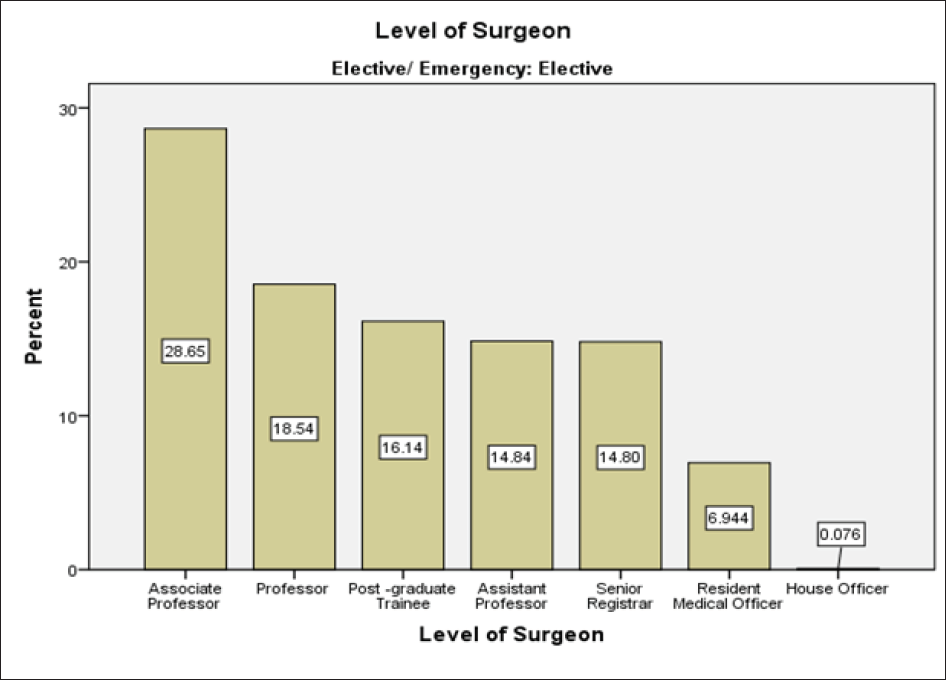
- Level of surgeon in elective surgeries.
| Level of a surgeon in an emergency | Frequency | Percent |
|---|---|---|
| Postgraduate Trainee | 1725 | 70.2 |
| Senior Registrar | 301 | 12.2 |
| Resident Medical Officer | 253 | 10.3 |
| Assistant Professor | 84 | 3.4 |
| Professor | 37 | 1.5 |
| House Officer | 32 | 1.3 |
| Associate Professor | 26 | 1.1 |
| Total | 2458 | 100.0 |
DISCUSSION
It is quite an observation that different cities have different diseases, also from one neighborhood to another, due to various social environments and ethnic grounds because of genetic factors. Environmental factors have a significant impact on diseases.[11]
Our total number of admission was 5079 in two years. These are the patients who underwent surgery, excluding those admitted for conservative management and observing and proceeding, which makes around 2540 patients in one year if we divide total number of patients in two years by 2.
A study shows that in Pakistan Institute of Medical Sciences (PIMS) Hospital Islamabad in 2016, 822 patients were operated on in a year.[12] Also, a prospective study was done in the Department of General Surgery (Ward 02), Jinnah Postgraduate Medical Centre and Karachi. The study had 3638 patients who underwent surgery in four years, from November 2011 to October 2015. During the 1st year, there were 840 cases which underwent surgery.[13] Another general surgical department unit 3 study from a civil hospital showed 779 patients admitted in a year.[11] A previous study in 2005 was reported from Abbasi Shaheed Hospital, which stated that 881 patients were admitted in a year, of which 449 underwent elective surgery and 315 underwent emergency surgery. 115 were managed conservatively.[14]
Among the studies mentioned, male patients’ pre-dominance was present; a similar finding has been reported in our survey: about 59.6% were males.
In our study, the most commonly performed elective surgical procedure was cholecystectomy 26.8%, followed by inguinal hernia repair 24.2%. Similar findings have been observed in another study conducted at two tertiary care hospitals in Islamabad, which showed that the most commonly performed elective general surgical procedure was laparoscopic cholecystectomy (46.5%), followed by direct inguinal hernia (29.8%).[15]

- Level of surgeons in emergency surgeries.
| Unit of the surgery department | Frequency | Percent |
|---|---|---|
| Surgical Unit 1 | 1812 | 35.7 |
| Surgical Unit 2 | 2007 | 39.5 |
| Surgical Unit 3 | 1260 | 24.8 |
| Total | 5079 | 100.0 |
| Elective/emergency | Frequency | Percent |
|---|---|---|
| Elective | 2621 | 51.6 |
| Emergency | 2458 | 48.4 |
| Total | 5079 | 100.0 |
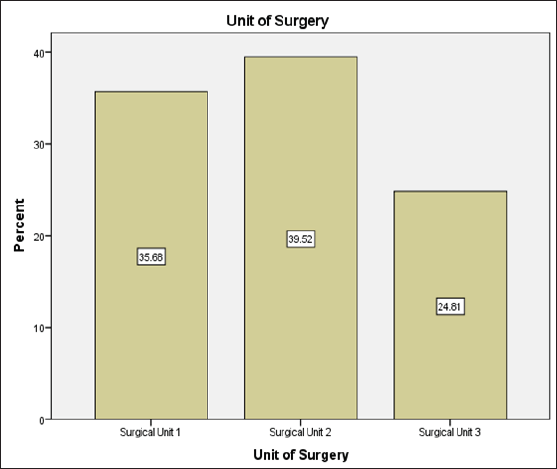
- Surgeries performed in respective departments.
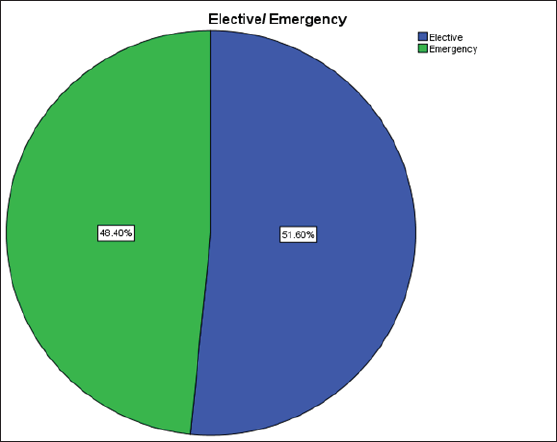
- Frequency of elective and emergency surgeries.
In another study total of 104 emergency surgeries were performed, with appendicectomy being the most common procedure in patients 32.7% followed by incision and drainage (26.0%) and laparotomy (20.2 %) in patients.[16] Meanwhile our study shows Incision and drainage was the most common emergency procedure (39.4%), followed by appendicectomy (33.0%) and exploratory laparotomy (15.9%). In the United Kingdom, the most commonly performed emergency procedures were appendicectomy (13.1%), endoscopy (11.3%), and drainage of skin lesions (9.7%) observed in 2016 in National health services hospital.[17]
Most of the surgeries in an emergency were performed by postgraduate trainees, around 70.2%. A retrospective study over 5 years in a district general hospital in London included 640 patients observed for complications, peri-operative survival figures and 5-year survival figures concerning the grade of the primary surgeon, and the results showed a similar type and number of complications for consultants and surgeons in training except for injury to ureters and anastomotic strictures were more familiar with the surgeries done by consultants. 5-year survival rate was more or less same for consultant and trainee surgeon.[18]
Another study from the United States of America showed that the involvement of trainee surgeons affects morbidity, mortality and operating time significantly (p-value < 0.001)[19] Another study showed that the participation of trainees had prolonged surgery time, but there were no significant adverse outcomes due to trainee involvement.[20]
Training sessions should take place to give the basic knowledge of audit to all healthcare workers and make them understand the importance of data and research for the development of a better healthcare system.[21]
Study shows that data collected by a medical professional was so accurate and of good quality, which helped the hospital to keep their data up to date in the future.[22]
After the literature review of our country, it is very alarming to see such scarce data available. A dire need is sensed to incorporate the clinical audit in our health care system to assess our proper demographics, disease spectrum, the pattern of admissions, details of procedures, length of hospital stay, complete data of morbidity and mortality and outcomes. It is therefore long due; a befit organized clinical audit should be made compulsory regularly for good clinical practice and beneficial for patients and clinicians. The modern practice of surgery requires regularly based audits to outshine previous practices. Like the developed countries, we should have systems and audit services available.
CONCLUSION
We have a higher number of elective surgeries as compared to emergency surgeries. Consultants have performed most of the elective surgeries—emergency surgeries mostly by residents and senior registrars. We have zero mortalities in our elective surgeries in comparison with emergency surgeries. We call attention to conducting continuous audits at our hospitals and all levels of health care and demand from higher authorized personnel to incorporate audit awareness into our teaching. Also, a proper database should be installed with updated records maintenance to improve the lack of health care.
Acknowledgment
None.
Ethical Approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patients consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Surgical audit of cases admitted at surgical unit I of Civil Hospital Karachi. Annals of PIMS ISSN. 2016;1815:2287.
- [Google Scholar]
- Audit of surgical emergency at Lahore General Hospital. J Ayub Med Coll Abbottabad. 2015;27:74-7.
- [PubMed] [Google Scholar]
- Evidence-based. medicine and the reconfiguration of medical knowledge. J Health Soc Behav 2004:177-93.
- [PubMed] [Google Scholar]
- Dutch Surgical Colorectal Cancer Audit Group. Evaluating national practice of preoperative radiotherapy for rectal cancer based on clinical auditing. Eur J Surg Oncol.. 2013;39:1000-6.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical audit in retina 2016: Chairman’s introduction. Eye. 2017;31(Suppl 2):S1.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- An evaluation of the POSSUM surgical scoring system. Br J Surg. 1996;83:812-5.
- [CrossRef] [PubMed] [Google Scholar]
- The evolution of auditing: An analysis of the historical development. J Account Audit. 2008 Dec 1;4:1.
- [Google Scholar]
- Audit of general surgical unit: Need for self evaluation. Pak J Surg. 2007;23:141-4.
- [Google Scholar]
- Surgical. audit of patients at a Tertiary Care Hospital. J. Islamabad Med. Dent. Coll. 2017;6:100-3.
- [Google Scholar]
- Compliance and effectiveness of WHO surgical safety checklist: A JPMC audit. Pak J Med Sci. 2016;32:831.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Surgical audit of Unit II, Department of Surgery, Abbasi Shaheed Hospital, Karachi. Ann Abbasi Shaheed Hosp Karachi Med Dent Coll. 2006;11:54-8.
- [Google Scholar]
- Audit of pre-operative antibiotic prophylaxis usage in elective surgical procedures in two teaching hospitals, Islamabad, Pakistan: An observational cross-sectional study. PloS one. 2020;15:e0231188.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- On-call emergency workload of a general surgical team. J Emerg Trauma Shock. 2009;2:15.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Emergency general surgery in the United Kingdom: a lot of general, not many emergencies, and not much surgery. J Trauma Acute Care Surg. 2018;85:500-6.
- [CrossRef] [PubMed] [Google Scholar]
- Elective and emergency surgery for colorectal cancer in a district general hospital: impact of surgical training on patient survival. Ann R Coll Surg Engl. 1989;71:370.
- [PubMed] [PubMed Central] [Google Scholar]
- Surgical resident involvement is safe for common elective general surgery procedures. J Am Coll Surg. 2011;213:19-26.
- [CrossRef] [PubMed] [Google Scholar]
- The impact of surgical trainee participation on sinus surgery outcomes. Laryngoscope. 2016;126:316-21.
- [CrossRef] [PubMed] [Google Scholar]
- An audit of clinical training exposure amongst junior doctors working in Trauma & Orthopaedic Surgery in 101 hospitals in the United Kingdom. BMC Med Educ. 2018;18:1-11.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- How accurate is a computerized surgical audit when resident medical staff collect the data? Aust N Z J Surg. 1992;62:563-8.
- [CrossRef] [PubMed] [Google Scholar]




