

Translate this page into:
Ureteric Rupture: Rare Complication of Inappropriate Urinary Bladder Catheterization
Address for correspondence Neeraj Kumar, MD, Department of Radiodiagnosis, Dr. Rajender Prasad Government Medical College Tanda, Kangra 176001, Himachal Pradesh, India (e-mail: dr.neerajchaudhary525@gmail.com).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
We have reported case of 71-year-old male with acute urinary retention due to gross prostatomegaly. Due to inappropriate catheterization, urinary bladder remained distended and ultimately caused left ureteric rupture. This article is peculiar as it shows that misplaced Foley's catheter may also lead to exceedingly rare complication of ureteric rupture and highlights importance of proper management of difficult catheterization which is otherwise considered a simple procedure.
Keywords
hematuria
inappropriate Foley's catheterization
prostatomegaly
ureteric rupture

Introduction
Ureteric rupture is rare and can be traumatic or nontraumatic. Previously reported common causes of ureteric rupture include trauma, urinary calculi, malignancy, and iatrogenic causes. However, ureteric rupture due to bladder outlet obstruction is exceedingly rare. We have reported case of elderly male having prostatomegaly who presented with acute urinary retention but inappropriate Foley's catheterization caused persistently raised intraluminal pressure, resulting ureteric rupture.
Case Report
A 71-year-old male presented to emergency department with history of inability to pass urine for 12 hours. Patient was catheterized in ambulance after which he started having bleeding per urethra but urine was not drained.
On physical examination, his vitals were stable, but he was in distress. Tenderness in left lumbar region and left renal angle. Renal function tests were normal. Contrast-enhanced computed tomography (CECT) abdomen revealed extravasation of contrast adjacent to left upper ureter and pelviureteric junction on excretory phase. There was also presence of left perinephric stranding. Urinary bladder was overdistended. Prostate was enlarged measuring 50.4 × 64.2 × 55.4 mm3 (volume = 93.7 cc). It was noted that Foley's catheter has coiled in anterior urethra and inflated Foley's bulb was also present in urethra (►Figs. 1 and 2). Patient received emergency double-J stenting of left ureter along with broad spectrum antibiotics. Nephrostomy catheter of 8 French (Fr) was placed in renal pelvis. Indwelling urinary bladder catheter was left in place for 3 weeks. Follow-up ultrasonography after 5 days showed disappearance of perinephric and periureteric collection. Patient condition gradually improved, and he was discharged 10 days after admission. Double-J stent was removed after 8 weeks.

- (A) Sagittal contrast-enhanced computed tomography (CECT) image showing overdistended urinary bladder, enlarged prostate and dilated Foley's bulb in urethra (solid white arrow). (B) Axial CECT image showing enlarged prostate. (C and D) Axial CECT images showing dilated Foley's bulb and coiled Foley's catheter in urethra.
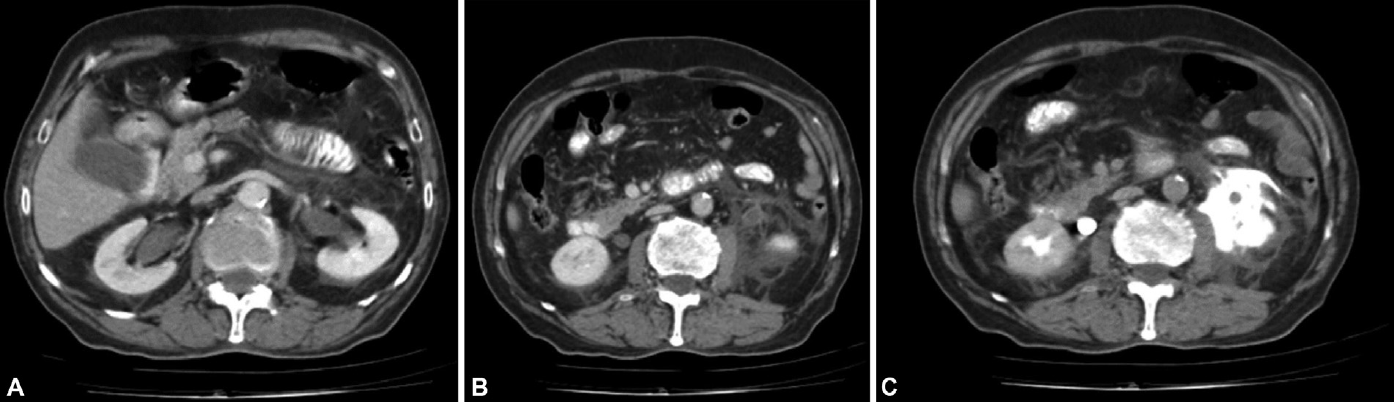
- (A) Axial contrast-enhanced computed tomography (CECT) image showing prominent bilateral renal pelvicalyceal system due to bladder outlet obstruction. (B) Axial CECT image showing left perinephric collection, stranding and thickening of left anterior renal and lateral conal fascia. Bilateral ureters are prominent with enhancement of left ureteric wall. (C) Axial excretory phase CECT image showing extravasation of contrast in left upper periureteric region.
Discussion
Foley's catheterization is commonly done to relieve acute urinary retention and prostatic hyperplasia is most common cause of urinary retention in adult male patients.1 There are several complications of catheterization ranging from urinary tract infections, genital infection, such as epididymitis, urethral bleeding, urethritis, urethral stricture, bladder stones, and others.2 Misplaced Foley's catheter leading to dilation of Foley's bulb in urethra is a “never event.” But this complication is still seen as urinary bladder catheterization is common procedure and is usually done by subordinate staff especially in developing countries where there is lack of professionally qualified medical and paramedical staff. Dilation of Foley's bulb in urethra may lead to urethral bleeding and rupture. We have presented this case in which it has ultimately led to ureteric rupture. Case of misplaced Foley's catheter leading to ureteric rupture has not been reported earlier.
Causes of ureteric rupture may be classified into spontaneous, traumatic, and obstructive. Traumatic causes include iatrogenic injury, penetrating injury, or blunt abdominal trauma. Obstructive causes include ureteric stones, abdominal or pelvic mass, and bladder outlet obstruction. Computed tomography (CT) urography is investigation of choice for ureteric rupture and to look for its possible cause.3
Conclusion
In conclusion, we have reported case of 71-year-old male who had gross prostatomegaly leading to acute urinary retention. Patient was catheterized by paramedic in ambulance to relieve obstruction but marked prostatomegaly and use of smaller sized (12 Fr) Foley's catheter led to curling of prostate in urethra. Since obstruction was not relieved in time, persistently dilated urinary bladder resulted in rupture of left ureter due to back pressure. This case was peculiar as timely drainage of acute urinary retention may have prevented ureteric rupture. It also highlights that misplaced Foley's catheter may even lead to serious and rare complication of ureteric rupture.
Few points to be remembered for prevention of intraurethral Foley's catheter balloon inflation and its complications as follows:
Foley's catheter should pass smoothly while inserting. Undue force should not be applied while inserting as it may lead to urethral rupture and coiling of catheter in urethra.
Catheter ≤12 Fr have higher chances of coiling in difficult catheterization.4 Therefore, Foley's catheter of ≥14 Fr should be preferred for male catheterization.
In case of urethral stricture, small feeding tube may be used.
Difficult catheterization may be done by railroading catheter over guidewire or under flexible cystoscope guidance.
If per urethral approach fails, then suprapubic cystostomy is used. However, in less experienced hands, suprapubic insertion of small-bore needle (21 G) can be used to aspirate 200 to 300 mL urine to buy time for suprapubic catheterisation.5
Seniors should be called for assistance during difficult catheterization.
Note
This research was carried out at Dr. Rajender Prasad Government Medical College, Tanda, Kangra, Himachal Pradesh, India.
Conflict of Interest
None declared.
Funding
None.
References
- Male urinary retention. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2010.
- [Google Scholar]
- Catheterization: possible complications and their prevention and treatment. Int J Urol. 2008;15(06):481-485.
- [CrossRef] [PubMed] [Google Scholar]
- A rare case of upper ureter rupture: ureteral perforation caused by urinary retention. Korean J Urol. 2012;53(02):131-133.
- [CrossRef] [PubMed] [Google Scholar]
- The risk of intra-urethral Foley catheter balloon inflation in spinal cord-injured patients: lessons learned from a retrospective case series. Patient Saf Surg. 2016;10(01):14.
- [CrossRef] [PubMed] [Google Scholar]




