

Translate this page into:
Epidemiology and Treatment Outcome of Blast Injuries to the Hand at a Tertiary Hospital of Kashmir Valley, India
*Corresponding author: Junaid Khurshid, MBBS, MS Surgery, Registrar, Department of Plastic and Reconstructive Surgery, SKIMS, Srinagar 190010, India. epidoctor2022@gmail.com, junaidk22@gmail.com
How to cite this article: Khurshid J, Bashir SA, Rasool A, Kulkarni OS. Epidemiology and treatment outcome of blast injuries to the hand at a tertiary hospital of Kashmir valley, India. Int J Recent Sur Med Sci, doi: 10.1055/s-0043-1762569
Abstract
Background
Blast injuries to hand can have disastrous consequences on account of loss of critical hand functions. This study was conducted to study the epidemiology and outcome of hand blast injuries reporting to emergency department of a tertiary care hospital.
Materials and Methods
All the blast injuries to hand admitted at our center between 2016 and 2020 were assessed at the time of injury and at 6 weeks after completion of primary management. The severity of injury and functional outcome was assessed using modified hand injury severity score (HISS) and quick disabilities of the arm, shoulder and hand (QuickDASH) scale, respectively. Descriptive statistics was calculated and correlation between HISS and DASH was assessed using Pearson's correlation coefficient.
Results
A total of 26 cases with a mean age of 23.12 ± 9.1 years were included. The subjects included 25 males and 22 subjects had injury to their dominant hand. The grade of injury was severe in 12 (46.15%) cases followed by moderate in 5 (19.2%) cases and major in 5 (19.2%) cases. The mean HISS score at injury was 67.46 ± 37.6. The mean QuickDASH score at follow-up was 37.24 ± 29.7. QuickDASH score at follow-up had a significant correlation with HISS score at baseline with a Pearson's correlation coefficient of (r = 0.67, p = 0.0012)
Conclusions
Blast injuries to hands are primarily seen in young males with low-grade explosives being the primary source of injury. Dominant hand is most commonly involved with many cases needing revascularization procedures. Higher severity of blast injuries to hand is associated with poor outcome at follow-up.
Keywords
Blast Injury
Hand
Hand injury severity score
QuickDASH score

Introduction
Hand injuries are the one of the most common musculoskeletal injuries encountered in emergency wards.[1,2] An increased surge has been seen secondary to the use of machines, fireworks, and violence-related cases.[3,4] Injuries are varied and can be combined with injuries to other areas of the body.[5] In addition, the severity is varied so is the intervention ranging from conservative management to amputation.[6,7] Patients with acute hand injury experience a temporary or permanent loss of hand functions and keeping in view the specific functions of hands, loss of these functions can have a varied impact in the quality of life both in short and long term.[8,9] Isolated blast injuries to the hands are usually seen in the civilian population as a result of accidental explosions of firecrackers or fireworks, gunshot injuries, and handling of a low-grade explosive like tear gas shells.[7,8] The extent of injury depends on the closeness or the proximity of the hand and also on the size of the explosive. Blast injuries present with a wide range of wounds, that is, laceration, avulsion, amputation, burn, vascular, compartment syndrome, crush injury, and degloving injury. Blast injuries can have disastrous consequences.[7] The pattern of isolated hand injuries is quite different from those of large scale blast injuries as these usually happen on account of low-grade explosives or firecrackers.[10] The predominance of hand involvement in such injuries is due to accidental blast during hurling a bomb as well as the injury sustained when a person tries to shield himself from a bomb being hurled at him with his hands.[11] To date, there are few studies that have investigated the epidemiology and outcome of blast injuries to hand in Kashmir Valley.
To address these research gaps, we investigated the pattern, etiology, and outcome of blast hand injuries reporting to the plastic surgery department of the sole specialized plastic surgery department in Kashmir Valley.
Materials and Methods
Study design/setting
This was a single-center study conducted at the plastic surgery department of SKIMS in Srinagar, India. The hospital is a tertiary hospital and a sole specialized center for specialized plastic surgery services in Kashmir Valley of India. Kashmir is a landlocked valley in the northeast of main Himalayan range. There have been instances of use of low-grade explosives like tear gas shells/stun shells to disperse the protestors. The most cases of isolated hand injuries in our studies were reported on account of use of these low-grade explosives that is a distinguishing feature in our study in comparison to studies in other parts of India, where firecrackers are the primary sources of isolated hand blast injuries. The study followed a cross-sectional design in which all patients reporting isolated blast injuries to hand from 2016 to 2020 were included.
Study participants
The participants were included from the accident and emergency department of the same hospital and participants who fit the inclusion criteria were included in the study. The initial management was provided the attending doctor and the attending doctor referred the case to plastic surgery department after initial conservative management. The information was recorded at the initial contact and patient was followed up on as per the hospital protocol. The outcome was assessed after 6 weeks of final management. Subjects who did not report for the final follow-up even after two telephonic contacts were excluded from the study.
Inclusion criteria
Patients who only if they had a blast injury primarily to hands; (ii) did not have any significant involvement of any other body part apart from hands, and (iii) reported to the health facility within 12 hours of the injury and had not underwent any major intervention to hand prior to reporting at the health facility were included in the study.
Exclusion criteria
Patients with any significant injury to any other part of body that impacted the management of hand injury and patients in whom any reconstructive management had been undertaken prior to reporting at the hospital were excluded from the study.
Assessment of injury and outcome
Modified hand injury severity score (HISS) was used to assess the severity of injury and quick disabilities of the arm, shoulder and hand (QuickDASH) score to assess the functional outcome.
Modified hand injury severity score
It is a descriptive scoring system specific to hand injuries and is widely used in clinical practice. Multiple previous studies have validated the scale and other studies have correlated higher score with poor outcomes. The injuries are graded into four categories: minor (< 20 points), moderate (21–50 points), severe (51–100 points), and major (≥ 101 points).[12,13] A higher score signifies greater severity of injury. All injuries were graded using the HISS checklist by a trained surgeon who was not involved in assessing the functional outcome that was done by a different surgeon to avoid bias.
QuickDASH
It is a shortened version of the DASH outcome measure and uses 11 items instead of the 30 items in the DASH outcome score. The shortened version enables faster measurement of disability and symptoms and has been validated for the use for outcome assessment after hand injuries. The score measures physical function and symptoms in persons with any musculoskeletal disorder of the upper limb. The scale has a main section comprising of 11 questions and 2 four-item optional module. The QuickDASH is scored in two components: the disability/symptom section (11 items, score 1–5) and the optional high-performance sport/music or work modules (4 items, score 1–5). We used only the disability/symptom section comprising of 11 items. A higher score signifies greater disability.[14-16]
Statistical methods
The data was entered on standard patient schedules and then entered in excel. Means and percentages were calculated using standard formulas. HISS score for each patient was calculated using excel tool. QuickDASH score for each item was summed and averaged, producing a score of five. The value was then transformed to a score out of 100 by subtracting one and multiplying by 25. This transformation is a standard process for QuickDASH scale and is done to make the score easier to compare.[16] Correlation between HISS and QuickDASH was assessed using Pearson's correlation coefficient.
Results
We included a total of 26 cases of isolated blast injuries to hand in our study. Two subjects were excluded as they were lost to follow-up. The participants had a mean age of 23.12 ± 9.1, with age ranging from 10 to 54 years. Only one subject was a female with the rest 25 being males. The most common source of injury was tear gas shells 16 (61.5%), followed by stun shells 5 (19.2%) and firecrackers 3 (11.5%). Dominant hand was affected in 22 (84.62%) of cases. Fracture of any hand or wrist bone was present in 19 (73.08%) cases with 8 (30.77%) and 7 (26.92%) cases requiring any revascularization surgery and amputation respectively. Table 1 describes the sociodemographic and clinical profile of the study participants.
Variable |
Value |
n |
% |
HISS Mean ± SD |
QuickDASH Mean ± SD |
|---|---|---|---|---|---|
Age of subject |
Mean ± SD |
23.12 ± 9.1 |
67.46 ± 37.6 |
37.24 ± 29.7 |
|
Age of subject |
10–19 years |
7 |
26.92 |
44.86 |
15.57 |
20–29 years |
15 |
57.69 |
78.60 |
46.66 |
|
30–39 years |
2 |
7.69 |
80.00 |
43.5 |
|
40–49 years |
1 |
3.85 |
68.00 |
63 |
|
50–59 years |
1 |
3.85 |
33.00 |
9 |
|
Gender |
Male |
25 |
96.15 |
68.72 |
38.4 |
Female |
1 |
3.85 |
36.00 |
8 |
|
Residence |
Rural |
21 |
80.77 |
68.66 |
37.8 |
Urban |
5 |
19.23 |
62.40 |
34.8 |
|
Cause of injury |
Tear gas shell blast |
16 |
61.54 |
74.62 |
42.5 |
Stun shell |
5 |
19.23 |
69.00 |
38 |
|
Firecracker blast |
3 |
11.54 |
27.66 |
4.66 |
|
Mobile phone |
1 |
3.85 |
85.00 |
62 |
|
Pressure cooker |
1 |
3.85 |
47.00 |
22 |
|
Injury to dominant hand |
Yes |
22 |
84.62 |
73.22 |
42.41 |
No |
4 |
15.38 |
35.75 |
8.75 |
|
Comorbidity |
Yes |
2 |
7.69 |
73.5 ± 57.28 |
42 ± 46.66 |
No |
24 |
92.31 |
66.96 |
36.83 |
|
Severity of injury (HISS grade) |
Minor (≤ 20 points) |
4 |
15.38 |
2 |
|
Moderate (21–50 points) |
5 |
19.23 |
11.4 |
||
Severe (51–100 points) |
12 |
46.15 |
40.3 |
||
Major (≥ 101 points |
5 |
19.23 |
75.8 |
||
Any associated fractures |
Yes |
19 |
73.08 |
77.92 |
46.15 |
No |
7 |
26.92 |
28.14 ± 12.31 |
6.42 ± 5.1 |
|
Revascularization done |
Yes |
8 |
30.77 |
81.00 |
40.8 |
No |
18 |
69.23 |
61.44 |
35.61 |
|
Amputation |
Yes |
7 |
26.92 |
99.14 |
60.75 |
No |
19 |
73.08 |
55.78 |
25.36 |
|
Abbreviations: HISS, hand injury severity score; QuickDASH, quick disabilities of the arm, shoulder and hand; SD, standard deviation.
Severity of injury
The mean HISS score at the initial assessment was 67.46 ± 37.6. The most common grade of injury was severe in 12 (46.15%) cases followed by five cases of major and moderate grade each. Only four cases (15.38%) presented with minor injury (HISS score ≤ 20).
Functional outcome at follow-up
The mean QuickDASH score at follow-up was 37.24 ± 29.7. The QuickDASH at follow-up was significantly associated with the HISS score with higher scores seen with higher HISS score (r = 0.67, p = 0.0012). QuickDASH was not significantly associated with age and cause of injury. Figure 1 depicts the correlation between HISS and QuickDASH scores.
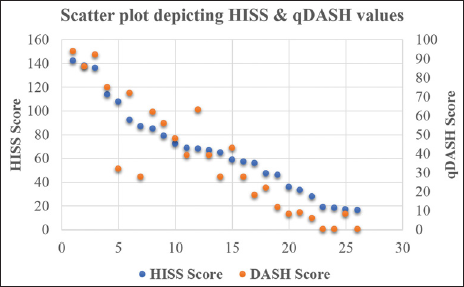
- Scatter plot depicting correlation between hand injury severity score (HISS) and quick disabilities of the arm, shoulder and hand (QuickDASH) scores.
Discussion
Our study describes the pattern of blast injuries to hand and their treatment outcome from a single tertiary care hospitals of Kashmir Valley, India, between 2016 and 2020. Our study includes 26 participants that met the inclusion criteria and included 25 males and a single female participant who had a firecracker-related blast injury to hand. We employed validated tools to describe the extent of injury as well as the functional outcome after the surgery. More than two-third participants had a severe or major blast injury to any hand and around three-fourth had an associated fracture of any hand or wrist bone. Revascularization/reimplantation was done in eight participants with seven subjects needing amputation of any part of the hand. The average QuickDASH score at follow-up was 37.24 ± 29.7. QuickDASH score at follow-up was positivity correlated with HISS score at the time on injury meaning higher grade injuries tend to have a long-term functional impairment.
The most common source of injury was tear gas shells (61.5%), followed by stun shells (19.2%) and firecrackers (11.5%). Mobile phone and pressure cookers were the sources of blast for one case each. The study area saw few events of political protests during these years in which tear gas and stun shells were used by administration to control protests. Low-grade explosives like tear gas stun shells are considered to be a nonlethal method of crowd control and sometimes the protestors try to handle these low-grade explosives during which the same may explode while in hand and lead to blast injuries of hand. In studies conducted in other parts of India, firecrackers are the most common source of injury.[10,17]
The subjects who reported with any blast hand injuries were primarily young males as most subjects were males aged less than 30 years. The primary reasons for the same could be the fact that most study participants had injuries due to handling of tear gas/stun shells during political protests in the study area. Participation in these protests is primarily from males and specifically young males which puts them at risk of blast injuries. The findings are similar to other studies as other studies have also found males to be more commonly affected than females.[1,8]
As the handling of these low-grade explosives is primarily done by the dominant hand, it tends to be the most commonly involved hand. In our study, dominant hand was involved in 84% of cases. This finding is in agreement with multiple other studies.[17,18] Greater dependence on dominant hand for routine activities means that functional outcome after recovery is very important for ensuring no or very limited residual disability.
Hands are integral components of almost all human functions ranging from routine work to highly specialized activities as most skills are expressed by intricate use of hand movements. Any long-term disability can be devastating and severely impair one's quality of life and capacity to lead to a socially and economically productive life. The QuickDASH at follow-up was significantly associated with the HISS score with higher scores seen with higher HISS score (r = 0.67, p = 0.0012). Higher severity of injury has been shown to be associated with poor outcome in multiple other studies also.[12,16]
Conclusion
Blast injuries to hands are primarily seen in young males with low-grade explosives being the primary source of injury. Dominant hand is most commonly involved with many cases needing revascularization procedures. It often results in long-term functional disability. The QuickDASH at follow-up was significantly associated with the HISS score with higher scores seen with higher HISS score.
Acknowledgement
The authors would like to thank all the technical staff from our department who provided invaluable support for the study and the patients for devoting their time and effort.
Ethical clearance
Ethical clearance was provided by the institutional review board of SKIMS Medical College, Srinagar, India.
Funding
This article is an original research article employing a cross-sectional study design. The article has not been previously published nor is submitted elsewhere for publication. All the authors have contributed reviewed and agree with its contents. The authors have no affiliations that can impact the results of the study. The authors have no funding sources to declare.
Conflict of interest
None declared.
References
- Outline of hand and wrist injuries presenting to an emergency of a tertiary care centre in Nepal. 2019. J Nepal Health Res Counc. 17:340-4. https://pubmed.ncbi.nlm.nih.gov/31735929/ [cited 2022 Dec 4]
- [Google Scholar]
- Epidemiology of hand and wrist injuries treated in a reference specialty center over a year. 2021. Acta Ortop Mex. 35:429-35. https://pubmed.ncbi.nlm.nih.gov/35451252/ [cited 2022 Dec 4]
- [Google Scholar]
- Hand injury prevention in India: are we doing enough? Indian J Plast Surg. 2011;44:532.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Common causes and types of hand injuries and their pattern of occurrence in Yekatit 12 Hospital, Addis Ababa, Ethiopia. Pan Afr Med J. 2019;33:142.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Demographic profile of hand injuries in an industrial town of north India: a review of 436 patients. Indian Journal of Surgery. 2012;75:454-61.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Reconstruction of blast injuries of the hand and upper limb. Injury. 2013;44:305-12.
- [CrossRef] [PubMed] [Google Scholar]
- Severe hand injuries from fireworks: injury patterns, outcomes, and fireworks types. J Hand Surg Am. 2017;42:385.e1-e8.
- [CrossRef] [PubMed] [Google Scholar]
- Blast injury to the hand: assessing the injury pattern and functional outcome of the thumb. 2021. Plast Reconstr Surg Glob Open. 9:e3767. https://pubmed.ncbi.nlm.nih.gov/34584822/ [cited 2022 Dec 4].
- [Google Scholar]
- Complex Injuries of the Hand - Tahseen Cheema - Google Books [Internet]. [cited 2022 Dec 4]. Accessed January 21, 2023 at: https://books.google.co.in/books?hl=en&lr=&id=5reHAwAAQBAJ&oi=fnd&pg=PA,183&dq=loss+of+hand+functions+blast+injuries+to+hand&ots=IbhRTG2wYe&sig=zrcFR48LIGcWRYTKm7DVr72KmHU&redir_esc=y#v=onepage&q=loss%20of%20hand%20functions%20blast%20injuries%20to%20hand&f=false
- Prevalence and patterns of cracker blast injuries of the hand. 2016. International Surgery Journal. 3:831-6. http://www.ijsurgery.com
- [Google Scholar]
- Firecracker injuries during Diwali festival: the epidemiology and impact of legislation in Delhi. Indian J Plast Surg. 2012;45:97-101.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Outcome of hand trauma: the hand injury severity scoring system (HISS) and subsequent impairment and disability. 2016;28B(4):295–9.
- [Google Scholar]
- Patient-reported quality of life and hand disability in elderly patients after a traumatic hand injury - a retrospective study. 2019. Health Qual Life Outcomes. 17:1-10. https://hqlo.biomedcentral.com/articles/10.1186/s12955-019-1215-9 [cited 2022 Dec 4]
- [Google Scholar]
- The use of disabilities of the arm, shoulder, and hand questionnaire in rehabilitation after acute traumatic hand injuries. 2007. J Hand Ther. 20:49-55, quiz 56. https://pubmed.ncbi.nlm.nih.gov/17254908/ [cited 2022 Dec 4]
- [Google Scholar]
- The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet Disord. 2003;4:11.
- [CrossRef] [PubMed] [Google Scholar]
- A retrospective cohort study of QuickDASH scores for common acute trauma conditions presenting for hand therapy. J Hand Ther. 2017;30:41-8.
- [CrossRef] [PubMed] [Google Scholar]
- Blast injuries to the hand: pathomechanics, patterns and treatment. J Emerg Trauma Shock. 2013;6:29-36.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Prevalence and patterns of cracker blast injuries of the hand. 2016. International Surgery Journal. 3:831-6. https://mail.ijsurgery.com/index.php/isj/article/view/191
- [Google Scholar]




