

Translate this page into:
Evaluation of Breast Masses by Sonomammography and X-ray Mammography in Correlation with Histopathological Findings
Corresponding Author: Namita S Chandak, Resident, Department of Radiodiagnosis, Jawaharlal Nehru Medical College, Wardha, Maharashtra, India, Phone: +919881675449, e-mail: chandaknamita76@gmail.com
This article was originally published by Thieme Medical and Scientific Publishers Private Ltd. and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Chandak NS, Dhande R. Evaluation of Breast Masses by Sonomammography and X-ray Mammography in Correlation with Histopathological Findings. Int J Recent Surg Med Sci 2017;3(1):3-6.
Abstract
Introduction:
Breast lumps are common presenting complaints in the female surgical outpatient department, which are due to varied breast pathologies. Breast infection most commonly affects women aged 18 to 50 years; in this age group, it can be divided into lactational and nonlactational infections. The process can affect the skin overlying the breast, where it can be a primary event, or it may be secondary to a lesion, such as sebaceous cyst or hidradenitis suppurativa.
Aim:
The aim of this article was to find out sonographic features of benign and malignant masses and correlate X-ray mammography and sonographic findings with histopathology with classification of all breast lesions according to the breast imaging reporting and data system final assessment categories (BI-RADS) (mammography).
Materials and methods:
This was a prospective diagnostic study conducted on 50 female patients from September 2015 to August 2016 in the Department of Radiodiagnosis in a tertiary care hospital.
Results:
In benign lesion, 24 (48%) of the patients had fibroadenoma, 2% intraductal papilloma, and 1 (2%) each had galactocele and tubercular abscess; in malignant lesion, 23 (46%) had ductal malignancy.
Conclusion:
The ultrasound features are helpful in differentiating benign from malignant masses. Classification of the lesions according to BI-RADS helps to improve the management of lesions.
Keywords
Breast masses
Correlation
Mammography
Ultrasonography.

INTRODUCTION
Breast lumps are common presenting complaints in the female surgical outpatient department, which are due to varied breast pathologies. Breast infection most commonly affects women aged 18 to 50 years; in this age group, it can be divided into lactational and non-lactational infections. The process can affect the skin overlying the breast, where it can be a primary event, or it may be secondary to a lesion, such as sebaceous cyst or hidradenitis suppurativa.1,2
Breast masses can be broadly classified as benign or malignant. Common causes of a benign breast mass include fibrocystic disease, fibroadenoma, cyst, galactocele, and abscess. Malignant breast disease encompasses many histologic types that include infiltrating ductal or lobular carcinoma and in situ ductal or lobular carcinoma. The main concern of many women presenting with a breast mass is the likelihood of cancer; however, most breast masses are benign.
In our study, an attempt is made to evaluate various breast masses using ultrasonography (USG) and mammography and histopathological correlation separately or in combination, to describe suitable indications, advantages, and limitations of each technique and differentiate the benign breast lesions from the malignant ones.
MATERIALS AND METHODS
This was a prospective analytical study done from September 2015 to August 2016 in the Department of Radiodiagnosis in a tertiary care hospital. All patients with palpable breast lump, patients who were screened for lump, and all cases of nipple discharge were included in the study.
Exclusion Criteria
Patients who did not undergo sonography, extremely painful breast mass, fungating mass, and patient with bleeding dyscrasia were excluded.
RESULTS
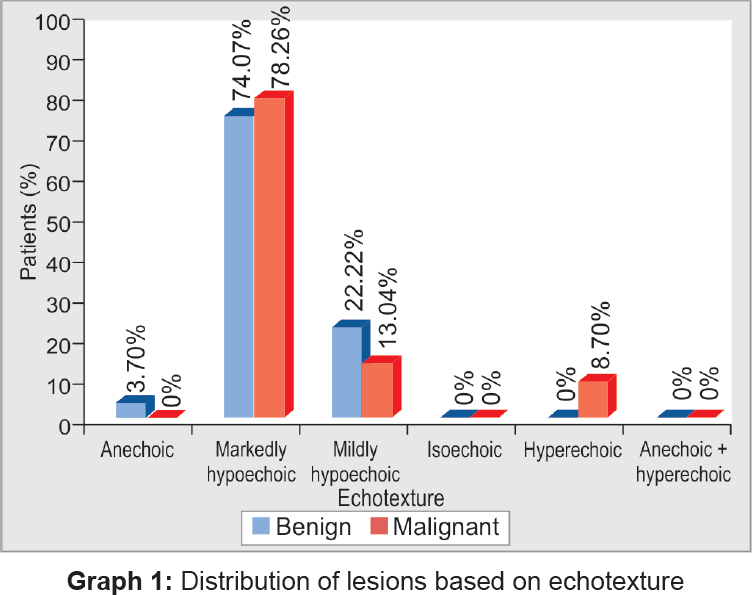
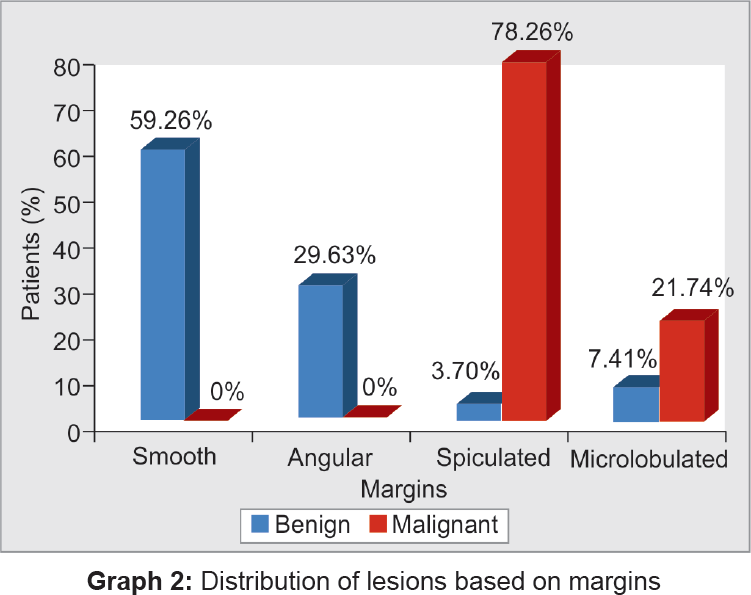
In this study, totally 50 patients complaining of breast mass in one or both breasts were examined clinically and evaluated with USG and mammography. All patients were abnormal and categorized according to the pathology and breast imaging reporting and data system final assessment categories (BI-RADS) classification (Table 1). Patients were in the age range of 11 to 70 years, with a mean of 38.54 years. It was found that the most benign lesions were seen in the younger age group (1st–2nd decades) as compared with that of the malignant lesions (3rd–7th decades). The mean age of the patients with benign lesions is 31.60 years, which is lower, and the mean age for malignant lesions is 47.36 years, which is higher. In the present study, most of the lesions ([19/50] and [21/50]) are located in the upper outer quadrant and upper inner quadrant respectively. About 78.26% of the malignant lesions were markedly hypoechoic (Graph 1). Smooth margins were noted in 92% of the benign lesions, which are more than findings of Cole-Beuglet et al,3 where 75% of benign lesions showed smooth margins (Graph 2). In the present study, 92% of the benign lesions showed posterior enhancement (Graph 3). The lesions were confirmed on histopathology (fine-needle aspiration cytology) (Graph 4), where maximum number of cases came out to be fibroadenoma. Few of the cases from our study are described (Figs 1 to 4).



- A 45-year-old female came for USG; transverse USG image reveals a typical larger transverse than anteroposterior diameter, homogeneous echotexture, and a posterior enhancement
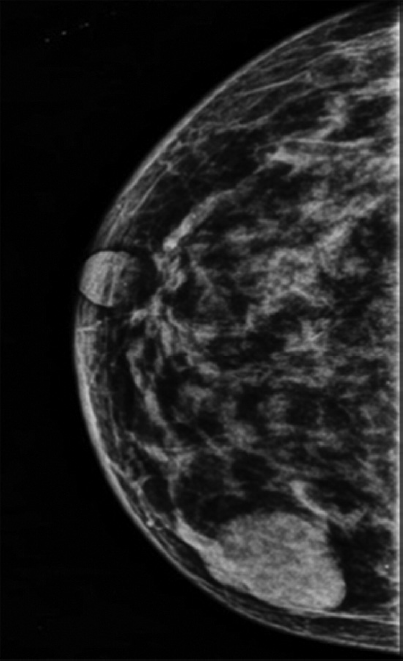
- A 45-year-old female came for screening mammogram; mammogram shows well-defined, smooth, marginated, rounded soft tissue density radiopacity in lower outer quadrant

- A 52-year-old woman with no personal or family history of cancer; mammogram showed a well-circumscribed mass with microcalcifications

- Malignant lesions. Transverse scan USG shows a typical malignant lesion, i.e., taller than wide, with hypoechoic echotexture with irregular spiculated margins
| BI-RADS | Lesions |
|---|---|
| Normal | 0 (0%) |
| Benign | 27 (100%) |
| Probably benign | 0 (0%) |
| Suspicious abnormalities | 0 (0%) |
| Highly suggestive of malignancy | 23 (100%) |
| Total | 50 (100%) |
DISCUSSION
The USG and mammography play an integral part in the evaluation and treatment of breast masses. These advances have allowed better delineation of various descriptive characteristics of breast masses.
The present study was conducted in the Department of Radiodiagnosis, which characterized 50 breast lumps in 50 female patients.
Age
The present study included the patients in the age group of 11 to 70 years, with a mean of 38.54 years. It was found that the most benign lesions were seen in the younger age group (1st–2nd decades) as compared with that of the malignant lesions (3rd–7th decades).
The mean age of the patients with benign lesions is 31.60 years, which is lower, and the mean age for malignant lesions is 47.36 years, which is higher. This finding is similar to the study by Skaane and Engedal4 who found the mean age of 39 years (18–81 years) for benign and 64 years (28–88 years) for malignant lesions.
Similar results were found by Naz and Malik,5 who concluded that the predominance of benign lesions in young patients ranges between 15 and 30 years and malignant lesions in older patients above 50 years.
In the present study, the youngest patient to have a malignancy was 31 years of age, whereas the oldest patient to have a benign lesion was 60 years of age. This finding is similar to the study by Huges and Courtney,6 who found that breast cancer is uncommon below the age of 35 years, the incidence increasing rapidly between the ages of 35 and 50; a slight bimodal trend in the age distribution has been observed with a dip in incidence at the time of menopause; breast cancer occurs a decade earlier in Indian women than in Western women. The mean age of occurrence is 42 years in India as compared with 53 years in White women.
Examination Findings
Location of the Lump
In the present study, most of the lesions ([19/50] and [21/50]) are located in the upper outer quadrant and upper inner quadrant, which is similar to a study by Singh et al,7 who concluded that 54% of the lumps were present in the outer upper quadrant of the breast.
MARKED HYPOECHOGENICITY
Markedly hypoechoic lesions should be defined as less echogenic than the relatively homogeneous medium-level echogenicity of the surrounding fat. More useful information can be gained by comparing lesion echogenicity to a structure that has an echogenicity near the middle of the gray-scale spectrum. In the breast, periductal elastic tissue, terminal ductal lobular units, and fat have an echogenicity near the medial of the gray-scale spectrum. Of these, fat is uniformly present in all patients; therefore, fat is the tissue against which the echogenicity of solid lesions can most consistently be compared from patient to patient.
In the present study, 78.26% of the malignant lesions were markedly hypoechoic. Similarly, Stavros et al8 found that two-thirds of the malignant lesions (66.66%) were markedly hypoechoic compared with fat.
It was concluded that even though marked hypoechogenicity is a worrisome finding for malignancy, isoechogenicity/mild hypoechogenicity are not necessarily reassuring and should be considered as indeterminate findings. Chao et al9 found 60% of the malignant lesions to be markedly hypoechoic and Hong et al10 found 62% of the malignant lesions to be markedly hypoechoic.
Skaane and Engedal4 and Popli11 in their studies have mentioned marked hypoechogenicity as a feature of malignancy.
GRAY-SCALE SONOGRAPHIC CRITERIA FOR BENIGNITY
Smooth Margins
In the present study, smooth margins were noted in 92% of the benign lesions, which is more than the findings of Cole-Beuglet et al,3 where 75% of benign lesions showed smooth margins.
POSTERIOR ENHANCEMENT
In the present study, 92% of the benign lesions showed posterior enhancement, which is similar to the study by Chao et al,9 who found 44% benign lesions to show posterior enhancement.
Harper and Kelly-Fry12 found that the lesions to show posterior enhancement were more in favor of benignancy.
CONCLUSION
The ultrasound features are helpful in differentiating benign from malignant masses. Ellipsoid shape, wider than taller, and posterior enhancement with lateral edge shadowing are good predictors of benignity, whereas smooth margins is a poor predictor.
Microcalcification and spiculation/angular margins: Microlobulations are good predictors of malignancy, whereas posterior enhancement is a poor predictor. Classification of the lesions according to BI-RADS helps to improve the management of lesions.
CLINICAL SIGNIFICANCE
Classification of the lesions according to BI-RADS classification helps to improve the management of lesions.
Source of support:
Nil
Conflict of interest:
None.
REFERENCES
- ABC of breast diseases. Breast infection. BMJ. 1994;309(6959):946-949.
- [CrossRef] [PubMed] [Google Scholar]
- Outpatient treatment of non-lactational breast abscesses. Br J Surg. 1992;79(1):56-57.
- [CrossRef] [PubMed] [Google Scholar]
- Fibroadenoma of the breast: sonomammography correlated with pathology in 122 patients. AJR Am J Roentgenol. 1983;140(2):369-375.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis of sonographic features in the differentiation of fibroadenoma and invasive ductal carcinoma. AJR Am J Roentgenol. 1998;170(1):109-114.
- [CrossRef] [PubMed] [Google Scholar]
- Different appearances of brest masses on high frequency ultrasound. PakJSurg. 2012;28(1):65-69.
- [Google Scholar]
- Follow up of patients with breast cancer. Br Med J. 1985;290(6477):1229-1230.
- [CrossRef] [PubMed] [Google Scholar]
- The accuracy of ultrasound in diagnosis of palpable breast lumps. JK Sci. 2008;10(4):186-188.
- [Google Scholar]
- Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995;196(1):123-134.
- [CrossRef] [PubMed] [Google Scholar]
- Prospective sonographic study of 3093 breast tumors. J Ultrasound Med. 1999;18(5):363-370.
- [CrossRef] [PubMed] [Google Scholar]
- BI-RADS for sonography: positive and negative predictive values of sonographic features. AJR Am J Roentgenol. 2005;184(4):1260-1265.
- [CrossRef] [PubMed] [Google Scholar]
- Pictorial essay: sonographic differentiation of solid breast lesions. Indian J Radiol Imaging. 2002;12(2):275-279.
- [Google Scholar]
- Ultrasound visualization of the breast in symptomatic patients. Radiology. 1980;137(2):465-469.
- [CrossRef] [PubMed] [Google Scholar]




