

Translate this page into:
Obstructed Inguinal Littre’s Hernia: A Vague Presentation
How to cite this article: Kulkarni ND, Adhikari G, Jadhav GS. Obstructed inguinal littre’s hernia: A vague presentation. Int J Recent Sur Med Sci doi: 10.1055/s-0042-1755179
Abstract
Littre’s hernia (LH) is a very rare presentation in patients presenting with hernias. It is the presence of Meckel’s diverticulum (MD) in a hernia sac. However, it usually presents with obstruction or strangulation. We are reporting here a case of Littre’s hernia in a 42-year-old male patient who presented with an irreducible swelling in the left inguinal region. The diagnosis of an incarcerated indirect inguinal hernia was made preoperatively. Intraoperative finding was however an obstructed Littre’s hernia with Meckel’s diverticulum in a very uniquely appearing hernia sac. The patient was successfully managed by resection of the MD along with ileal segment, primary anastomosis, and mesh hernioplasty on the inguinal floor.
Keywords
Littre’s hernia
Meckel’s diverticulum
Obstructed inguinal Littre’ hernia
Incarcerated hernia

Introduction
Littre’s hernia (LH) is the protrusion of Meckel’s diverticulum (MD) through a potential abdominal opening with a container sac. It was originally defined as “the presence of a Meckel’s diverticulum in any hernial sac” by Reinke in 1841.[1] The entity was first described by Alexis Littre in 1700 as “ileal diverticula in the inguinal hernia.” However, the concept of “Littre’s hernia” was improved when Johann Friedrich Meckel in 1809 defined the true congenital diverticulum of the gut, which is now named after him.[2]
Littre’s hernia (LH) is defined as the protrusion of Meckel’s diverticulum (MD) through a potential abdominal opening with a container sac. It was first described by French physician Alexis Littre in 1700 while Reinke established the term in 1841.[1]
Among all the congenital gastrointestinal abnormalities, MD is the most common entity. A failure in the obliteration of the omphalomesenteric duct after the fifth week of gestation results in the formation of this true diverticulum with an independent blood supply. It is more prevalent in males (up to four times) with an incidence of up to 4%.[2] Littre’s hernia is a very rare complication of MD with an incidence as low as 1% of all cases and 0.9% in cases of incarcerated or strangulated hernias.[3]
Here, we report an interesting case of obstructed inguinal Littre’s hernia, which, to our surprise, presented in a very unique and vague way intraoperatively. Very few cases of obstructed LH have been reported before and we attempt to further enrich the available literature through this presentation.
Case Report
A 42-year-old adult male patient, farmer by occupation, presented in the casualty department with a chief complaint of left inguinal swelling and pain for 2 days. The onset of swelling was spontaneous, associated with discomfort that gradually became painful. The pain was sharp, severe in intensity, and radiating to the scrotum. There was no complaint of associated fever, nausea, or vomiting. Bowel habits were regular. There was no history of systemic illness or previous surgery. On examination, a pear-shaped swelling of size 6 × 4 cm approximately was noted in the left inguinal region. The swelling was firm and tender on palpation. There was no cough impulse and the swelling was irreducible both spontaneously and manually. Bilateral testes were normal and could be felt separately. No regional lymphadenopathy was noted. A diagnosis of incarcerated indirect inguinal hernia was considered. An emergency ultrasound was done that was suggestive of an obstructed inguinal hernia with the possibility of a bowel loop in the hernia sac. The patient was posted for emergency surgery under spinal anesthesia. An inguinal incision was taken and developed on the left side. On opening the external oblique aponeurosis, a tense, congested, bluish spherical mass of size 8 × 6 cm was seen in the inguinal canal. Further dissection exposed a thick, fibrosed “kidney-shaped” mass originating from the internal inguinal ring [Figure 1]. The incision was expanded above to avail full exposure of the mass and the inguinal floor. On further exploration, this peculiar mass was found to be a densely thickened hernia sac with a Meckel’s diverticulum and an obstructed ileal loop segment of length 10 cm approximately as its content [Figure 2]. MD along with the involved bowel loop was resected, and ileo-ileal end-to-end primary anastomosis was done in two layers. Tension-free Onlay mesh hernioplasty was done to re-strengthen the inguinal floor using a prolene mesh of size 7.5 × 15 cm. The patient recovered well in a span of 7 days postoperatively and was discharged in clinically stable condition on the eighth day. The histopathological report of the specimen confirmed the presence of Meckel’s diverticulum with the gastric mucosa.
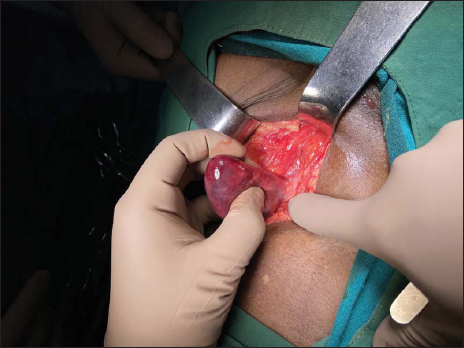
- A unique “kidney-shaped” mass seen originating from internal inguinal ring.

- Meckel’s diverticulum with Ileal segment resected.
Discussion
Clinically, MD remains silent in the majority of cases. It is classically seen on the antimesenteric border of the distal ileum roughly 2 feet proximal to the ileocecal junction containing gastric or pancreatic mucosa.[4] Per rectal bleeding, ulceration, bowel obstruction, or perforation are the complications of symptomatic MD in 5 to 17% of the cases.[5] The risk of incarceration in LH is more in the pediatric age group than in adults. Male gender and right-side preponderance have also been reported in a few studies.[1] LH appears most commonly through the inguinal region followed by the femoral and umbilical region respectively. Some studies in the literature however have suggested the femoral region as the most common.[6] True Littre’s is a common variety containing MD alone as the content of the hernia sac whereas mixed Littre’s hernia, as in this case report, contains a segment of the bowel along with MD.[7]
There are no specific clinical signs and symptoms to differentiate LH and other types of hernias. Clinical suspicion of LH can be made by asking for a history of rectal bleeding or noticing the presence of a fecal fistula in the hernia sac on a CT scan; however, literature has suggested that preoperative diagnosis of LH with imaging modalities is difficult and hence it is usually an intraoperative finding.[8] Symptoms in an incarcerated LH are typically late in onset because only the MD gets involved in the hernia sac initially rather than the ileal loop itself. If the ileal segment is involved, abdominal distention with other features of obstruction can be seen.
Diverticulectomy with wedge resection is the preferred surgical technique in uncomplicated cases of MD with viable bowel. If the base of MD appears to be edematous and inflamed or if the underlying ileal segment appears to be ischemic due to incarceration or strangulation, then segmental ileal resection with end-to-end bowel anastomosis is required.[9] Robjin et al, in 2006, suggested a risk scoring system for the management of incidentally found MD that included four criteria: male sex, age less than 45 years, diverticula length more than 2 cm, and the presence of a fibrous band.[10] In our case, we found that the length of MD was around 5 cm with edema and inflammation at the base. Also, the involved ileal segment appeared to be dusky in our case, the viability of which was in doubt even after giving 100% oxygen to the patient for more than 5 minutes. Hence, we proceeded with the option of ileal resection and anastomosis.
The presence of MD in an inguinal hernia alters the dynamics of the hernia surgery altogether. The “clean” surgery otherwise, now becomes a “clean-contaminated” entity as a result of which mesh placement becomes a challenging affair for the surgeon. The benefits of mesh hernioplasty versus the risk of recurrence in anatomical herniorrhaphy are debatable. With all due consideration, we decided to perform Lichtenstein’s tension-free repair using a non-absorbable prolene mesh in our case. Recent studies and trials have warranted the use of absorbable biological meshes in high-risk surgical fields; however, the availability in emergency settings and cost-bearing is an issue.[11] The World Society of Emergency Surgery (WSES) 2017 emergency hernia surgery guidelines advocated the use of permanent mesh in a “clean-contaminated” type of field in order of low risk of infection and prevention of the recurrence.[12]
Conclusion
A preoperative diagnosis of Littre’s hernia is difficult. A patient of pediatric age group, history of rectal bleeding, presence of incarcerated swelling may help a surgeon to suspect LH. Urgent surgery is the best approach in an irreducible/incarcerated or strangulated hernia with resection of Meckel’s diverticulum. The underlying ileal loop must be thoroughly checked and confirmed for its viability, or else bowel resection and anastomosis are mandatory. The decision to choose between mesh hernioplasty and anatomical repair for hernia defect repair chiefly rests on the surgeon’s personal experience. This particular case is interesting not only for the rare finding of obstructed LH but also for its vaguely presented hernia sac.
Conflict of interest
None declared.
References
- Right Inguinal Obstructed Littre’s Hernia in a Child. J Nepal Paedtr. Soc [Internet]. 2017;36:300-302.
- [CrossRef] [Google Scholar]
- “Reporte de un caso clínico,” Revista del hospital de niños de Buenos Aires Vol 55. 2013. p. :249-50.
- [Google Scholar]
- Littré’s hernia: a rare intraoperative finding. Cureus. 2020;12:e11065.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A rare case of a strangulated Littre’s hernia with Meckel’s diverticulum duplication. Case report and literature review. Int J Surg Case Rep. 2017;33:58-61.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- A rare cause of acute abdomen: perforation of double Meckel’s diverticulum. Case Rep Gastrointest Med. 2015;2015:648417.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Littré s hernia: unusual find in inguino-scrotal hernial repair. Rev Esp Enferm Dig. 2010;102:506-7.
- [CrossRef] [PubMed] [Google Scholar]
- Littre’s hernia: a systematic review of the literature. Hernia. 2019;23:125-30.
- [CrossRef] [PubMed] [Google Scholar]
- Littre hernia in childhood: a case report with a brief review of the literature. Afr J Paediatr Surg. 2011;8:221-4.
- [CrossRef] [PubMed] [Google Scholar]
- Management of incidentally found Meckel’s diverticulum a new approach: resection based on a risk score. Acta Chir Belg. 2006;106:467-70.
- [CrossRef] [PubMed] [Google Scholar]
- Absorbable meshes in inguinal hernia surgery: a systematic review and meta-analysis. Surg Innov. 2017;24:289-98.
- [CrossRef] [PubMed] [Google Scholar]
- A strangulated Meckel’s diverticulum in an inguinal hernia: a case report and literature review. Int Med Case Rep J. 2021;14:605-9.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]




